


To evaluate the association between degrees of nicotine dependence measured by the Fagerström test (FTCD) and different tests of motivation to stop smoking.
Material and methodsObservational study, multicenter conducted in smoking clinics in daily clinical practice. Demographics, smoking status, FTCD scores, and motivation test results were collected: Richmond test (TR), Henri Mondor Paris motivation test (HMP), Khimji–Watts test (KW), and the visual analog scale of motivation to stop smoking. The statistical analysis was descriptive, and correlation and analysis tests and regression models were used.
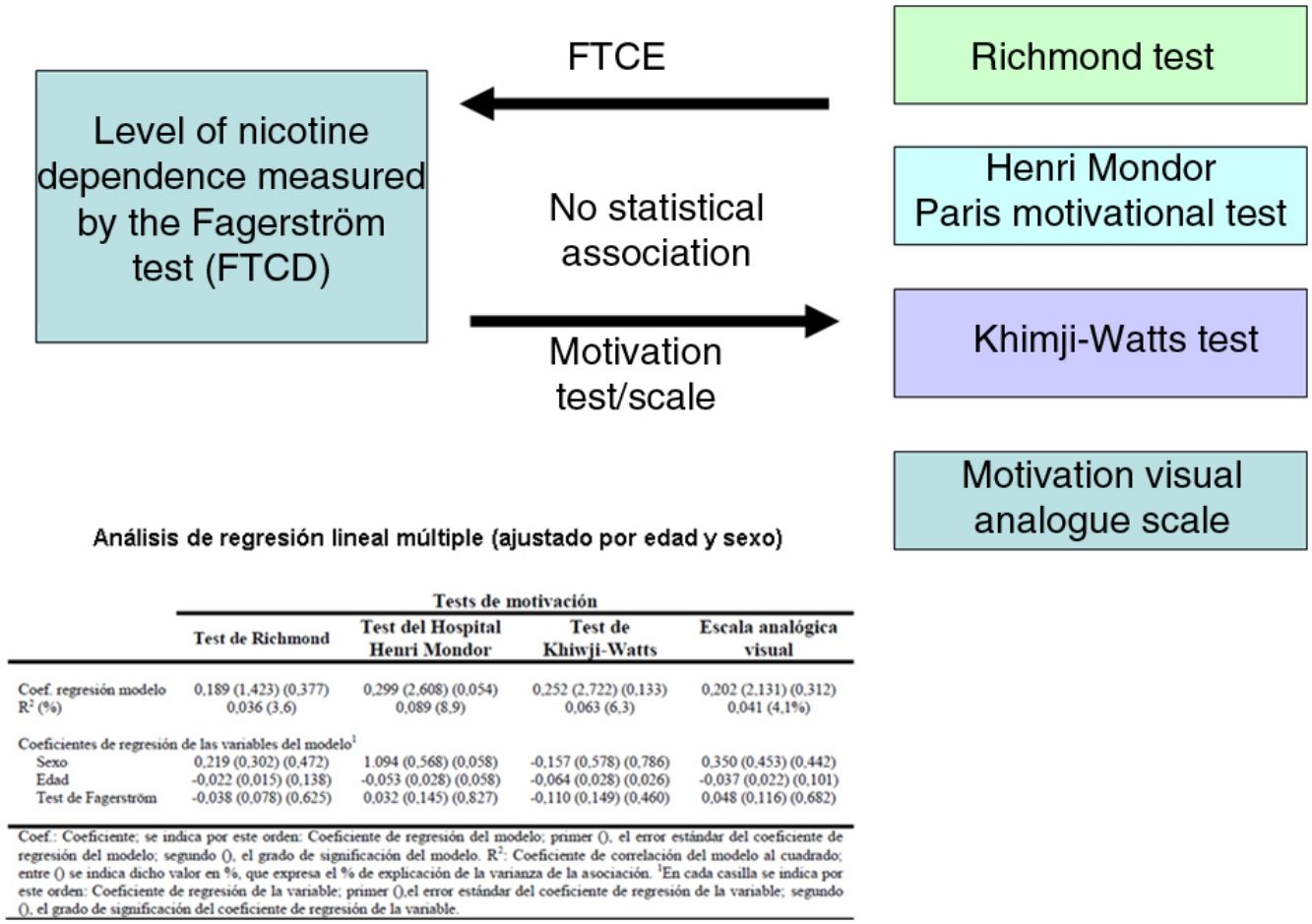
ResultsA total of 314 subjects were included [162 women (51.59%)]. Males smoked an average of 3.3 cigarettes/day more than women (95% CI: 0.9–5.6 cigarettes/day, P=0.006) and their cumulative consumption was 7.8 pack-years higher than in women (95% CI: 2.1–13.5 pack-years). We found no association between FTCD and the motivation tests to stop smoking used in this study.
ConclusionsWe found no association between the degree of dependence and the motivation to quit smoking measured by the aforementioned instruments.
Evaluar la existencia de asociación entre el grado de dependencia por la nicotina medido por el test de Fagerström (FTCD) y diferentes test de motivación para dejar de fumar.
Material y métodosEstudio observacional y multicéntrico realizado en consultas de tabaquismo en la práctica clínica diaria. Se recogieron variables demográficas, de estatus de fumador y las puntuaciones del FTCD y los test de motivación: test de Richmond (TR), test motivacional Henri Mondor de París (HMP), test Khimji-Watts (KW) y la escala analógica visual de motivación para dejar de fumar. El análisis estadístico fue descriptivo y se utilizaron test de correlación y análisis y modelos de regresión.
ResultadosFueron incluidos 314 sujetos (162 mujeres [51,59%]). Los varones fumaron en promedio 3,3cig/día más que las mujeres (IC95%: 0,9-5,6cig/día, p=0,006) y tuvieron un consumo acumulado superior a las mujeres en 7,8 años-paquete (IC95%: 2,1 a 13,5 años-paquete). No se encontró asociación entre el FTCD y los test de motivación para dejar de fumar empleados en este estudio.
ConclusionesNo hemos encontrado asociación entre el grado de dependencia y la motivación para dejar de fumar medidos por los instrumentos mencionados.
Success in stopping smoking depends on the balance between the individual's motivation to quit and their degree of nicotine dependence, and clinicians should be able to evaluate both aspects.1 The Fagerström Test for Cigarette Dependence (FTCD)2 is the most widely used tool for measuring nicotine dependence. It consists of 6 questions, and a score≥6 indicates a high level of dependence.3 Motivation to quit is important because the treatments that have been shown to help subjects stop smoking do not work as well in smokers who are not highly motivated.1 Motivation can be assessed qualitatively, by asking the smoker directly about their interest and intention to give up, and this approach often works in clinical practice.1 A semiquantitative method, the visual analog scale, can also be used, and quantitative methods1 are also available, including the Richmond test (RT), the Henri Mondor Paris test (HMP), and the Khimji–Watts test (KW). Motivation and the number of previous attempts to quit have been shown as predictors of effort, while a low level of dependence4,5 and a high level of self-efficacy6 have been shown to be predictors of abstinence after the attempt. When motivation is separated into its different components, “desire” and “intention” have been shown as independent predictors of the attempt to quit, while “duty” mitigates the predictive value of the previous two.7 Another aspect to bear in mind is that motivation and dependence are related: motivation varies over time and is heavily influenced by circumstances. When smokers tell us about their desire to quit in the clinical interview, they may not be accurately reflecting their true feelings.1
It has been reported that an increased motivation to change correlates negatively with the level of dependency, and that these factors, together with age, predict relapse.8 Gantiva et al.9 found a significant negative correlation between the level of dependency and motivation in a group of college students.
Our hypothesis is that subjects with greater reliance on nicotine are less motivated to stop smoking. The aim of this study was to evaluate the existence of an association between the degree of nicotine dependence measured by the FTCD and tests of motivation to quit smoking conducted in this study.
Materials and MethodsDesignThis was a multicenter, observational study conducted in routine clinical practice in 5 tertiary hospitals, 3 secondary hospitals, and a specialized smoking cessation unit, located in Spain and in the Republic of Argentina. Patients treated in these centers were included consecutively between October 1, 2014 and October 31, 2015.
Variables CollectedThe following variables were collected: sex, age, number of years smoking, daily consumption of cigarettes, accumulated consumption in pack-years, number of previous attempts to quit, number of attempts to quit in the past year, FTCD, the RT, HMP, and KW motivation tests, and the visual analog scale of motivation to quit smoking.
Ethics CommitteesThis study was submitted to each of the ethics committees of the participating medical centers, all of whom found it appropriate in terms of ethics and methodology, and provided certificates of approval.
Statistical AnalysisQuantitative variables were expressed as mean, standard deviation (SD), and range of values. Qualitative variables were expressed by absolute value and percentage. The Kolmogorov–Smirnov test was used to determine the normal distribution of quantitative variables for each sex category. Mean values were compared using the Student's t-test, after checking the assumption of homogeneity of variances of the distributions of the test for each category of sex using Levene's test of equality of variances. If the assumptions required by the Student's t-test were not met, the comparison between mean values was performed using the non-parametric Mann–Whitney U test and Welch's robust ANOVA.
The relationship between the degree of tobacco dependence as measured by the FTCD and the degree of motivation to quit smoking as measured by each of the motivation tests used was determined by calculating Pearson and Spearmann bivariate correlation coefficients (since, in most cases, the distributions do not follow a normal distribution). In cases where the correlations were statistically significant, the association was represented graphically using a scatter plot, and calculated using a simple linear regression analysis. A multivariate linear regression analysis was performed to analyze the association between FTCD, and motivation as measured by the various tests, controlling for age and sex. An α value<0.05 was considered statistically significant. The analysis was carried out using SPSS 15.0 for Windows (version 15.0.1 [22 Nov 2006], SPSS Inc., 1989–2006).
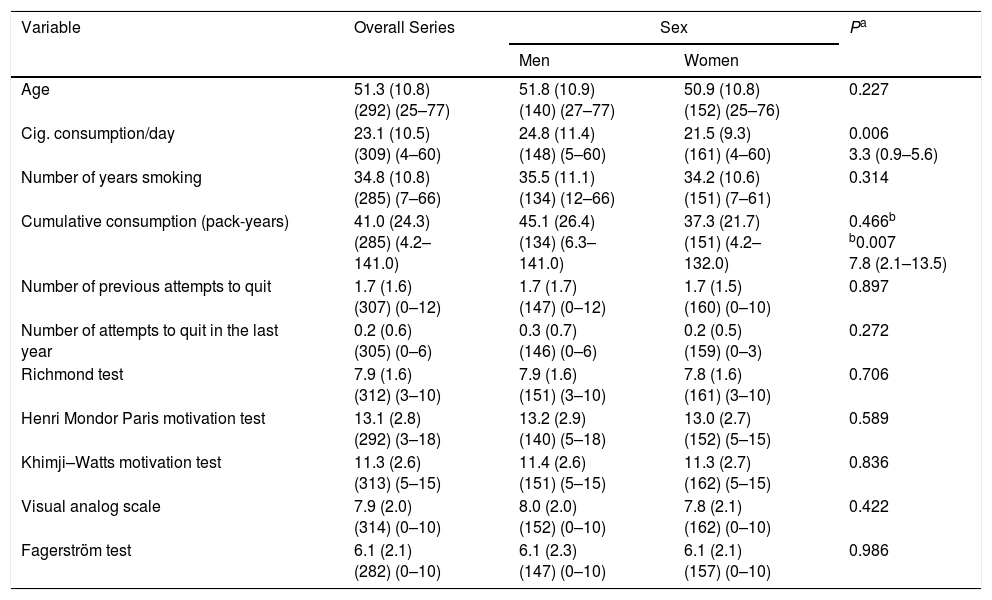
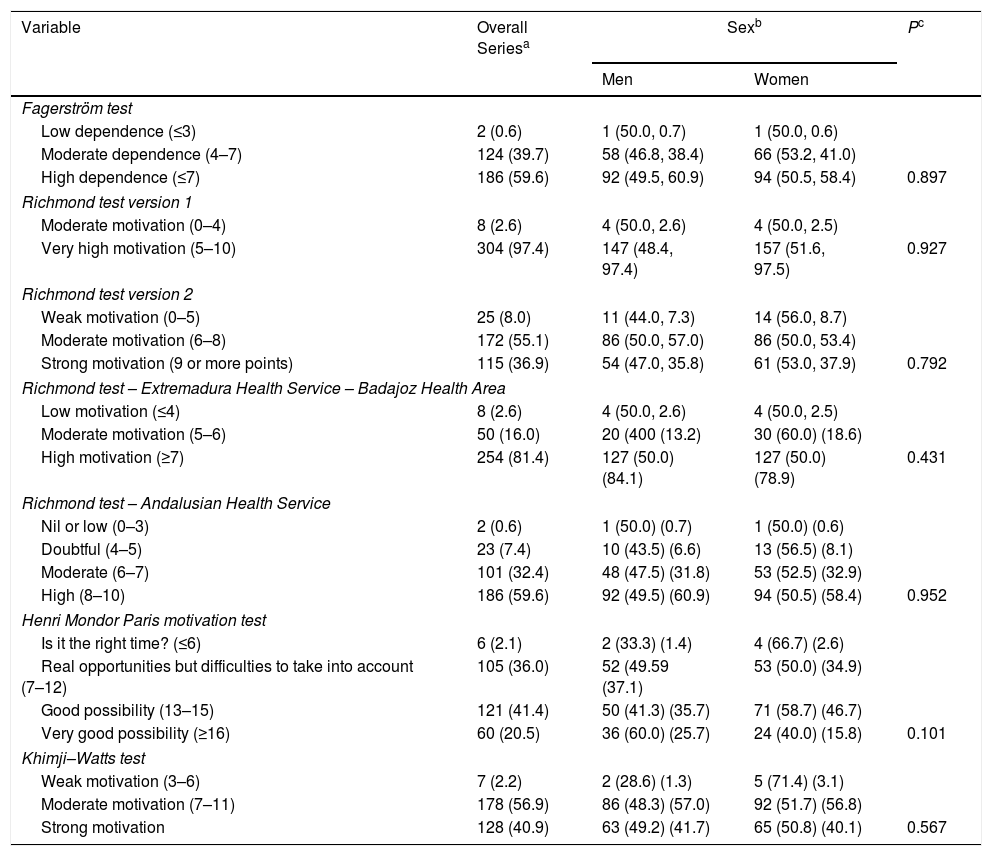
ResultsDescriptive AnalysisThe series included 314 subjects (162 women [51.59%]). Table 1 shows the mean values for quantitative variables, for the overall series and by sex, and the comparison between mean scores between the sexes. Table 2 shows the percentage values of qualitative variables for the overall series and by sex, and the comparison between men and women for each of these variables. In the absence of a defined cut-off point for high motivation, the analysis was performed using different categorizations of the same test (Table 2). Statistically significant differences between men and women were found in the amount of consumption expressed in cigarettes per day (cigs/day) and cumulative consumption of tobacco. Men smoked an average of 3.3 cigs/day (95% CI: 0.9–5.6 cigs/day, P=0.006) more than women. The variable “cumulative consumption of tobacco (pack-years)” showed statistically significant differences in the Student's t-test, but not in the Mann–Whitney non-parametric U test (P=0.466) that was used when the variable did not meet the assumptions of the Student's t-test; however, the difference in mean values between men and women was confirmed by Welch's robust ANOVA (P=0.007). On average, cumulative consumption among men was 7.8 pack-years higher than women (95% CI: 2.1–13.5 pack-years),
Mean Values of Quantitative Variables for the Overall Series and by Sex, and Comparison Between Men and Women.
| Variable | Overall Series | Sex | Pa | |
|---|---|---|---|---|
| Men | Women | |||
| Age | 51.3 (10.8) (292) (25–77) | 51.8 (10.9) (140) (27–77) | 50.9 (10.8) (152) (25–76) | 0.227 |
| Cig. consumption/day | 23.1 (10.5) (309) (4–60) | 24.8 (11.4) (148) (5–60) | 21.5 (9.3) (161) (4–60) | 0.006 3.3 (0.9–5.6) |
| Number of years smoking | 34.8 (10.8) (285) (7–66) | 35.5 (11.1) (134) (12–66) | 34.2 (10.6) (151) (7–61) | 0.314 |
| Cumulative consumption (pack-years) | 41.0 (24.3) (285) (4.2–141.0) | 45.1 (26.4) (134) (6.3–141.0) | 37.3 (21.7) (151) (4.2–132.0) | 0.466b b0.007 7.8 (2.1–13.5) |
| Number of previous attempts to quit | 1.7 (1.6) (307) (0–12) | 1.7 (1.7) (147) (0–12) | 1.7 (1.5) (160) (0–10) | 0.897 |
| Number of attempts to quit in the last year | 0.2 (0.6) (305) (0–6) | 0.3 (0.7) (146) (0–6) | 0.2 (0.5) (159) (0–3) | 0.272 |
| Richmond test | 7.9 (1.6) (312) (3–10) | 7.9 (1.6) (151) (3–10) | 7.8 (1.6) (161) (3–10) | 0.706 |
| Henri Mondor Paris motivation test | 13.1 (2.8) (292) (3–18) | 13.2 (2.9) (140) (5–18) | 13.0 (2.7) (152) (5–15) | 0.589 |
| Khimji–Watts motivation test | 11.3 (2.6) (313) (5–15) | 11.4 (2.6) (151) (5–15) | 11.3 (2.7) (162) (5–15) | 0.836 |
| Visual analog scale | 7.9 (2.0) (314) (0–10) | 8.0 (2.0) (152) (0–10) | 7.8 (2.1) (162) (0–10) | 0.422 |
| Fagerström test | 6.1 (2.1) (282) (0–10) | 6.1 (2.3) (147) (0–10) | 6.1 (2.1) (157) (0–10) | 0.986 |
Values are given follows: mean (standard deviation) (sample size) (range).
Cig.: cigarettes.
Frequency Distribution of Qualitative Variables for the Overall Series and by Sex, and Comparison Between Men and Women.
| Variable | Overall Seriesa | Sexb | Pc | |
|---|---|---|---|---|
| Men | Women | |||
| Fagerström test | ||||
| Low dependence (≤3) | 2 (0.6) | 1 (50.0, 0.7) | 1 (50.0, 0.6) | |
| Moderate dependence (4–7) | 124 (39.7) | 58 (46.8, 38.4) | 66 (53.2, 41.0) | |
| High dependence (≤7) | 186 (59.6) | 92 (49.5, 60.9) | 94 (50.5, 58.4) | 0.897 |
| Richmond test version 1 | ||||
| Moderate motivation (0–4) | 8 (2.6) | 4 (50.0, 2.6) | 4 (50.0, 2.5) | |
| Very high motivation (5–10) | 304 (97.4) | 147 (48.4, 97.4) | 157 (51.6, 97.5) | 0.927 |
| Richmond test version 2 | ||||
| Weak motivation (0–5) | 25 (8.0) | 11 (44.0, 7.3) | 14 (56.0, 8.7) | |
| Moderate motivation (6–8) | 172 (55.1) | 86 (50.0, 57.0) | 86 (50.0, 53.4) | |
| Strong motivation (9 or more points) | 115 (36.9) | 54 (47.0, 35.8) | 61 (53.0, 37.9) | 0.792 |
| Richmond test – Extremadura Health Service – Badajoz Health Area | ||||
| Low motivation (≤4) | 8 (2.6) | 4 (50.0, 2.6) | 4 (50.0, 2.5) | |
| Moderate motivation (5–6) | 50 (16.0) | 20 (400 (13.2) | 30 (60.0) (18.6) | |
| High motivation (≥7) | 254 (81.4) | 127 (50.0) (84.1) | 127 (50.0) (78.9) | 0.431 |
| Richmond test – Andalusian Health Service | ||||
| Nil or low (0–3) | 2 (0.6) | 1 (50.0) (0.7) | 1 (50.0) (0.6) | |
| Doubtful (4–5) | 23 (7.4) | 10 (43.5) (6.6) | 13 (56.5) (8.1) | |
| Moderate (6–7) | 101 (32.4) | 48 (47.5) (31.8) | 53 (52.5) (32.9) | |
| High (8–10) | 186 (59.6) | 92 (49.5) (60.9) | 94 (50.5) (58.4) | 0.952 |
| Henri Mondor Paris motivation test | ||||
| Is it the right time? (≤6) | 6 (2.1) | 2 (33.3) (1.4) | 4 (66.7) (2.6) | |
| Real opportunities but difficulties to take into account (7–12) | 105 (36.0) | 52 (49.59 (37.1) | 53 (50.0) (34.9) | |
| Good possibility (13–15) | 121 (41.4) | 50 (41.3) (35.7) | 71 (58.7) (46.7) | |
| Very good possibility (≥16) | 60 (20.5) | 36 (60.0) (25.7) | 24 (40.0) (15.8) | 0.101 |
| Khimji–Watts test | ||||
| Weak motivation (3–6) | 7 (2.2) | 2 (28.6) (1.3) | 5 (71.4) (3.1) | |
| Moderate motivation (7–11) | 178 (56.9) | 86 (48.3) (57.0) | 92 (51.7) (56.8) | |
| Strong motivation | 128 (40.9) | 63 (49.2) (41.7) | 65 (50.8) (40.1) | 0.567 |
Values in the columns “Men” and “Women” are as follows: absolute value; (percentage of the Fagerström test score, that is to say, reading the table by rows); (percentage by sex, that is to say, reading the table by columns). For example, of the 124 subjects with moderate dependency, 58 (46.8%) were men and 66 (53.3%) were women; in contrast, of the 151 men, 58 (38.4%) had a moderate level of tobacco dependence as measured by the Fagerström test, and of the 161 women, 66 (41.0%) had a moderate level of tobacco dependence.
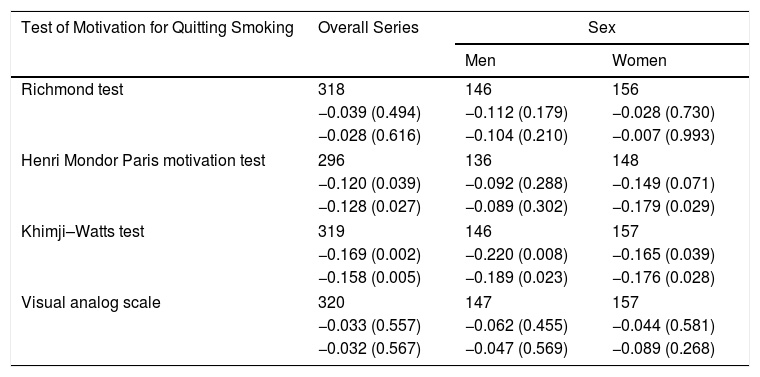
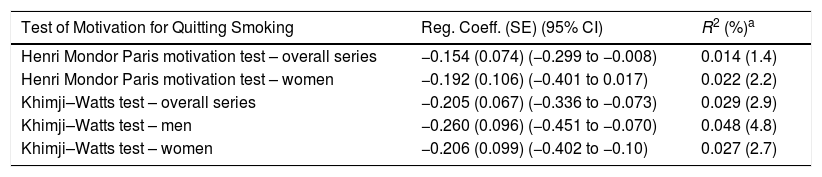
Table 3 shows the Pearson and Spearmann correlation coefficients between FTCD and the different tests of motivation to quit smoking collected in this study, both for the overall series and by sex. All the associations showed negative correlation coefficients, suggesting that the higher the tobacco dependence as measured by the FTCD, the lower the motivation to quit smoking; however, these associations were only statistically significant for the degree of motivation to quit smoking measured by the HMP (and in this case, only for women), and by the KW. Table 4 shows estimates of the regression coefficients of the linear regressions that demonstrate the association between FTCD and the tests of motivation to quit smoking with statistical significance, and the proportion of explained variance of that association. These associations are represented in graphs in Fig. 1. In all cases, the percentage of explained variance of the association between variables was very low (less than 55%).
Correlation Coefficients Between the Fagerström Test for Cigarette Dependency and Various Tests of Motivation to Quit Smoking.
| Test of Motivation for Quitting Smoking | Overall Series | Sex | |
|---|---|---|---|
| Men | Women | ||
| Richmond test | 318 | 146 | 156 |
| −0.039 (0.494) | −0.112 (0.179) | −0.028 (0.730) | |
| −0.028 (0.616) | −0.104 (0.210) | −0.007 (0.993) | |
| Henri Mondor Paris motivation test | 296 | 136 | 148 |
| −0.120 (0.039) | −0.092 (0.288) | −0.149 (0.071) | |
| −0.128 (0.027) | −0.089 (0.302) | −0.179 (0.029) | |
| Khimji–Watts test | 319 | 146 | 157 |
| −0.169 (0.002) | −0.220 (0.008) | −0.165 (0.039) | |
| −0.158 (0.005) | −0.189 (0.023) | −0.176 (0.028) | |
| Visual analog scale | 320 | 147 | 157 |
| −0.033 (0.557) | −0.062 (0.455) | −0.044 (0.581) | |
| −0.032 (0.567) | −0.047 (0.569) | −0.089 (0.268) | |
Sample size, Pearson's correlation coefficient (below), followed by Spearmann's correlation coefficient are indicated. Level of statistical significance indicated in brackets (p).
Estimates of the Regression Coefficients of the Linear Regressions Between the Fagerström Test for Cigarette Dependency and Tests of Motivation to Quit Smoking, With Statistically Significant Correlation.
| Test of Motivation for Quitting Smoking | Reg. Coeff. (SE) (95% CI) | R2 (%)a |
|---|---|---|
| Henri Mondor Paris motivation test – overall series | −0.154 (0.074) (−0.299 to −0.008) | 0.014 (1.4) |
| Henri Mondor Paris motivation test – women | −0.192 (0.106) (−0.401 to 0.017) | 0.022 (2.2) |
| Khimji–Watts test – overall series | −0.205 (0.067) (−0.336 to −0.073) | 0.029 (2.9) |
| Khimji–Watts test – men | −0.260 (0.096) (−0.451 to −0.070) | 0.048 (4.8) |
| Khimji–Watts test – women | −0.206 (0.099) (−0.402 to −0.10) | 0.027 (2.7) |
Reg. coeff.: regression coefficient; 95% CI: 95% confidence interval of the regression coefficient; SE: standard error of the regression coefficient.

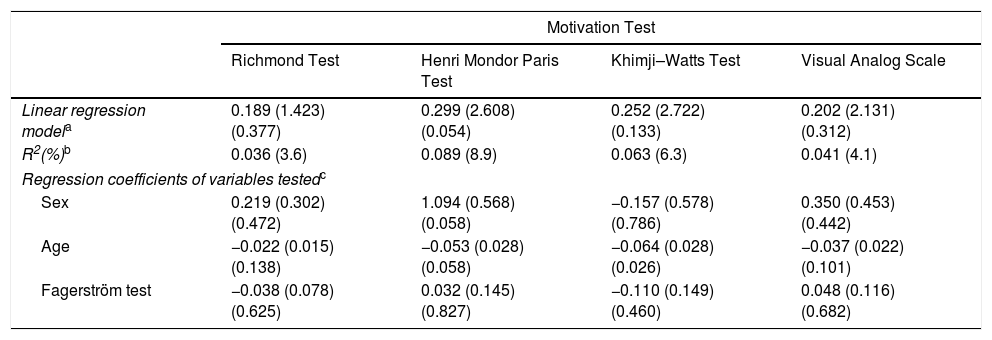
Table 5 shows the results of the various multiple linear regression analyses between FTCD and the different tests of motivation to quit smoking, controlling for sex and age. After controlling for age and sex, none of the models of association between FTCD and the various tests of motivation to quit smoking were statistically significant. Only in the case of the association between FTCD and motivation to quit smoking measured with the HMP did the relationship approach significance (P=0.054); but the FTCD variable was not significant (P=0.827).
Multiple Linear Regression Analysis Between the Fagerström Test for Nicotine Dependency Variable and the Motivation to Quit Smoking Measured by Various Tests.
| Motivation Test | ||||
|---|---|---|---|---|
| Richmond Test | Henri Mondor Paris Test | Khimji–Watts Test | Visual Analog Scale | |
| Linear regression modela | 0.189 (1.423) (0.377) | 0.299 (2.608) (0.054) | 0.252 (2.722) (0.133) | 0.202 (2.131) (0.312) |
| R2(%)b | 0.036 (3.6) | 0.089 (8.9) | 0.063 (6.3) | 0.041 (4.1) |
| Regression coefficients of variables testedc | ||||
| Sex | 0.219 (0.302) (0.472) | 1.094 (0.568) (0.058) | −0.157 (0.578) (0.786) | 0.350 (0.453) (0.442) |
| Age | −0.022 (0.015) (0.138) | −0.053 (0.028) (0.058) | −0.064 (0.028) (0.026) | −0.037 (0.022) (0.101) |
| Fagerström test | −0.038 (0.078) (0.625) | 0.032 (0.145) (0.827) | −0.110 (0.149) (0.460) | 0.048 (0.116) (0.682) |
Values are given as follows: regression coefficient of the model; (standard error of the regression coefficient of the model); (level of significance of model).
The most important finding of our study is that no association was observed between dependence measured by the FTCD and the various motivation tests. At this point, the question we must ask is whether the motivation tests really measure motivation to quit smoking. It is of the utmost importance to have health measurement scales that can be used in clinical practice and research, and it is imperative that these instruments undergo a validation process to ensure the quality of their measurements. This process consists of adapting the instrument to the cultural environment where it will be administered, and verifying its psychometric characteristics, including reliability, validity, sensitivity, and feasibility. If we are to use a scale with any degree of confidence, we must be sure that it provides an accurate and reliable measurement under the same circumstances, that it is sensitive to changes in the clinical situation, and that it is easy to use in practice. This process of testing the characteristics of an instrument is called validation.10 None of the motivation tests used in this study has been validated in their original language nor, of course, in Spanish (aside from language differences, there are cultural differences between different populations that make these procedures essential). In addition, the cut-off point indicating when motivation for quitting smoking can be considered high is unknown. An analysis of the psychometric properties of the FTCD confirmed its reliability for the assessment of nicotine dependence in different environments and populations.11 The FTCD was developed after the previous 10-question version showed psychometric disadvantages, low criterion validity and a multifactorial structure.12 Becoña and Vazquez13 studied a group of Galician smokers to assess the applicability of the Spanish version of the FTCD and its relationship with age, sex, and the consumption of cigarettes. The authors found that the value of the test increases with age and tobacco consumption, and that its value is greater in men than in women. The authors suggest that the Spanish version of the FTCD is useful for measuring dependency and identifying smokers with an increased risk of developing smoking-related diseases.
The widespread use of the different questionnaires used in this study has led them to be considered appropriate for measuring dependence and motivation. Richmond et al.14 conducted a study in a primary care setting to identify characteristics that predicted continuous abstinence in a group of smokers. In this study, they evaluated participants’ motivation to quit smoking by designing a rating scale, with a range of 0–10 (10: high motivation), based on the 4 questions that are currently included in the test known as the RT. In the discussion, the authors indicated that a significant proportion of smokers responded positively to the 4 questions of the RT, indicating that many of them wanted to quit smoking. Those who obtained the highest score in the scale were up to 4.5 times more likely to remain abstinent for 12 months than those with a minimum score. According to the authors, these results supported the robustness of this scale as a predictor of abstinence. The RT includes 2 questions that were previously used by Russell15 to determine the respondent's motivation to quit smoking, and these were used to build a simple model of smoking cessation based on the degree of motivation to quit smoking and on the degree of nicotine dependency among the smokers. The greater the motivation, the higher the chances of quitting smoking; and the greater the dependence, the lower the possibility.
The HMP motivation questionnaire is easy to complete and relatively short, but poorly validated.16 The HMP has been used in various studies to determine the degree of motivation to quit smoking,16–21 with low motivation categorized as a score of equal to or less than 12, and high motivation when the value is greater than 12. Layoun et al.,21 in a study to establish predictors of attempts to quit among Lebanese smokers, found that the HMP and FTCD showed acceptable reliability as measured by Cronbach's alpha statistic (HMP [0.757] and FTCD [0.789]), and that smokers with high motivation as measured by the HMP were twice as likely to quit smoking (P=0.007, OR=1.98; 95% CI: 1.21–3.26) In another study,20 the same group aimed to determine the predictors of prior attempt and time of abstinence, and found that a longer period of abstinence (more than one month) was associated with low dependence on nicotine and with high motivation as measured by the HMP; subjects with a high score on the motivation test were twice as likely to maintain a longer period of abstinence. Similarly, Mannocci et al.17 conducted a study aimed at determining whether the photographs and health alerts printed on cigarette packets helped achieve greater abstinence or a reduction in the number of cigarettes smoked, stratified by demographic characteristics, dependence on nicotine, and motivation as measured by the HMP. They found that the more motivated group of smokers was better informed than the less motivated group and believed that warnings on cigarette packets increased awareness and motivation to reduce consumption and quit smoking. All these studies cite La Torre et al.22 whenever the HMP test is mentioned; however, this reference is merely a review of the available tests for measuring motivation.
The KW test appears in a French website to help quit smoking (Tabac info Service, in French)23 which cites a study published in 199424 as the source of the test, but that has not been validated either. With regard to the analog scales, these have been considered by most authors as reliable and valid measurement tools, although they have their limitations.25 Lindberg et al.26 evaluated factors associated with smoking cessation and compared the characteristics and nicotine dependence of smokers with and without chronic obstructive pulmonary disease. The authors used analog scales to measure motivation and self-efficacy, and found that they were perfectly valid for discriminating between high or low motivation and self-efficacy.
It seems therefore that we can answer the question posed at the beginning of this discussion by saying that, with the exception of the KW (for which there is no written evidence), these motivation scales can distinguish between individuals with more chance of quitting or a greater number of attempts to give up, since this group scores higher in these scales. Motivation is key to change; it is a multidimensional, dynamic and fluctuating state that is interactive and can be modified: a patient's motivation may be affected by the personal style of their treating physician.27 All of these elements could explain why motivation to quit smoking measured by these tests has no correlation with the degree of nicotine dependence measured by the FTCD.
Another finding of our study was that the average daily consumption of cigarettes and the cumulative consumption of tobacco were higher in men than in women. This fact has already been established, as several previous studies have shown that men and women differ in their smoking habits: women smoke fewer cigarettes per day, start smoking later in life, and have a lower accumulated consumption, they tend to use cigarettes with a lower nicotine content, and do not inhale as deeply as men. Women smokers, moreover, become dependent quicker, and have serious difficulties giving up.28,29
Our study has some limitations. 1) The findings were obtained from a routine clinical practice population who came voluntarily to the smoking cessation clinic to make a serious attempt to quit smoking, and might not reflect the situation had these test scores been obtained from a general population of smokers. 2) The results cannot be extrapolated to the general population, and replicating this study in different scenarios and geographical locations could produce other results. 3) The use of questionnaires in patients is not always accurate due to potential problems in understanding the questions, or the possibility that some questions are understood implicitly, others are downplayed, and others are just omitted, which could result in certain information biases. 4) It has been established that the scores obtained on patient questionnaires differ, depending on whether they are administered by the healthcare professional or are self-administered, and the moment at which the information is collected should also be uniform, as this factor could also affect the final results. This variability could lead to different results.
We believe, therefore, that it would be advisable to perform a more ambitious study in a greater number of patients, in order to complement the information obtained in this study, and to confirm whether or not there is a relationship between the degree of dependency and the motivation to quit smoking.
In conclusion, we found no association between the degree of dependency and the motivation to quit smoking as measured with the tests used here, so the proposed hypothesis cannot be supported.
FundingThis study was supported with a SEPAR 2013 grant.
Conflict of InterestsThe authors state that they have no conflict of interests.
Please cite this article as: de Granda-Orive JI, Pascual-Lledó JF, Asensio-Sánchez S, Solano-Reina S, García-Rueda M, Martínez-Muñiz MÁ, et al. ¿Existe asociación entre el grado de dependencia por la nicotina y la motivación para dejar de fumar? Arch Bronconeumol. 2019;55:139–145.







