
As we enter the third year of the pandemic, the impact of COVID-19 on patients with pre-existing specific respiratory diseases remains poorly characterised, creating uncertainties for risk management and posing a challenge to delivery of safe, effective, evidence-based care.
Patients with severe alpha-1 antitrypsin deficiency (AATD) have increased risk of developing chronic, progressive lung disease, particularly pan-lobular emphysema.1 Pathogenesis is considered one of imbalance between the destructive proteolytic burden resulting from inhaled, pro-inflammatory factors and impaired defences arising from deficiency of alpha-1 antitrypsin (AAT). Increased risk from COVID-19 may be consequent to reduced pulmonary functional reserve and from overwhelmed, impaired anti-inflammatory defences by the cytokine/inflammatory storm associated with COVID-19.2,3 The likelihood of progressive respiratory failure and irreversible lung damage would be expected to be increased. AAT may also have a beneficial role in modifying the severity of COVID-19 through several different mechanisms.4
The EARCO ERS Clinical Research Collaboration5 sought, at the outset of the pandemic, to estimate the risk posed by COVID-19 to patients with severe AATD. Anonymised data on all known cases of COVID-19 in patients with severe AATD across participating countries was collated into a database to identify and ordinate risk factors for an adverse outcome. Patients age>18 years with severely reduced serum level of AAT due to two inherited pathological alleles in the SERPINA1 gene (PiZZ, PiSZ or rare variants with an equivalent serum AAT level (viz. <60mg/dl i.e. <11μmol/L)6 were included. Diagnosis of COVID-19 was based on a pathognomonic clinical presentation (± a positive confirmatory polymerase chain reaction test). Subjects were identified by EARCO reference centres through direct contact with patients attending the centre or patient contact prompted by information disseminated via national patient groups to their members. Details of patient baseline characteristics and outcome, including hospitalisation, treatment, mortality and spirometry (from historical records and post-acute COVID-19 measurements) were collected. Patients that were not admitted to hospital were assessed ‘virtually’ via phone contact and further data was obtained from hospital records. Ethics approval was obtained from HRA and Health and Care Research Wales (IRAS ID 285484). As a retrospective collection of fully anonymised clinical data from medical records, consent was not considered to be required.
Patient characteristics were compared according to genotype and outcome. Normality of distributions was assessed using the Kolmogorov–Smirnov test. For quantitative variables, the Student's t-test (Mann–Whitney U-test if normality was not assumed) or ANOVA tests (in the case of variables with more than 2 categories) were carried out. The Chi-squared test (Fisher test for frequencies<5) was used for comparison of categorical variables. A backward stepwise logistic regression analysis was performed to identify clinical variables related to poor outcome, defined as hospitalisation or death. p-Values<0.05 were considered statistically significant.
We identified 105 patients consecutively (65 male, 61%) across 21 centres in 10 countries with a mean (SD) AAT level of 32.8 (19.6) mg/dL, mean (SD) age of 51.3 (12.2) years, baseline FEV1%predicted (measured in 93 patients): 63.4 (31.0) %, (n=93), and PiZZ:PiSZ (or equivalent severity of deficiency) genotype distribution, 81:24. CT-evidenced emphysema was present in 66 (63%) patients and bronchiectasis in 5 (4.7%). Fourteen patients (14%) were receiving regular augmentation therapy. Non-respiratory comorbidities were present in 36 (34%) patients (19 [18%] hypertension, 4 [3%] diabetes, 12 [11%] liver, 2 [2%] renal and 3 [3%] cardiovascular disease). COVID-19 presentation (93 [88%] patients with positive PCR) included worsening breathlessness in 72 (68%) patients, cough in 75 (71%), anosmia and/or dysgeusia in 39 (37%), headache in 51 (49%), myalgia in 55 (52%) and gastrointestinal symptoms in 29 (28%). Hospitalisation occurred in 32 (31%) patients (mean duration, 12.9 [9.1] days), with intensive care admission required in 5 (4.8%) (mean duration, 5.6 [2.7] days), high flow oxygen in 21 (21%) and non-invasive ventilation/continuous positive airway pressure (NIV/CPAP) in 9 (9%). Poor outcome was more frequent in the PiZZ (29 patients, 35.8%) compared to the PiSZ (4 patients, 16.6%) group, although not significant (p=0.076). Four (3.8%) deaths occurred, all of them in PiZZ patients. Paired analysis of decline in FEV1%predicted showed an overall mean (SD) change of −1.8 (5.4) % (n=42, p=0.01) and changes of +1.3 (5.4) % (n=10, p=0.37) and −2.8 (4.7) %, (n=32, p=0.001) in the PiSZ and PiZZ groups, respectively. There was a median (IQR) interval of 167 (63–311) days between the time of ‘pre-COVID-19’ spirometry and onset of COVID-19 symptoms, 120 (84–178) days between symptom onset and ‘post-COVID-19’ spirometry and a median duration of acute illness of 16 (12–39) days (n=37). Regression analyses are shown in Table 1.
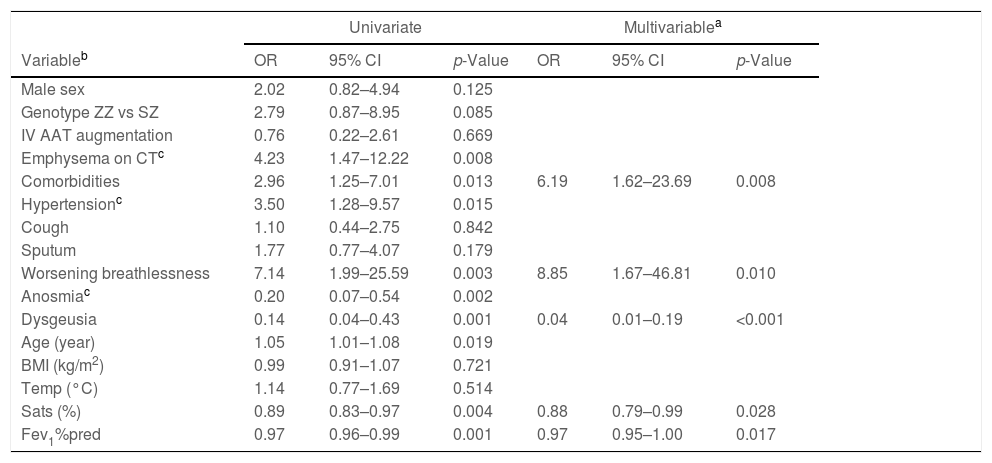
Multivariable logistic regression analysis for variables independently associated with poor outcome (N=105).
| Univariate | Multivariablea | |||||
|---|---|---|---|---|---|---|
| Variableb | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Male sex | 2.02 | 0.82–4.94 | 0.125 | |||
| Genotype ZZ vs SZ | 2.79 | 0.87–8.95 | 0.085 | |||
| IV AAT augmentation | 0.76 | 0.22–2.61 | 0.669 | |||
| Emphysema on CTc | 4.23 | 1.47–12.22 | 0.008 | |||
| Comorbidities | 2.96 | 1.25–7.01 | 0.013 | 6.19 | 1.62–23.69 | 0.008 |
| Hypertensionc | 3.50 | 1.28–9.57 | 0.015 | |||
| Cough | 1.10 | 0.44–2.75 | 0.842 | |||
| Sputum | 1.77 | 0.77–4.07 | 0.179 | |||
| Worsening breathlessness | 7.14 | 1.99–25.59 | 0.003 | 8.85 | 1.67–46.81 | 0.010 |
| Anosmiac | 0.20 | 0.07–0.54 | 0.002 | |||
| Dysgeusia | 0.14 | 0.04–0.43 | 0.001 | 0.04 | 0.01–0.19 | <0.001 |
| Age (year) | 1.05 | 1.01–1.08 | 0.019 | |||
| BMI (kg/m2) | 0.99 | 0.91–1.07 | 0.721 | |||
| Temp (°C) | 1.14 | 0.77–1.69 | 0.514 | |||
| Sats (%) | 0.89 | 0.83–0.97 | 0.004 | 0.88 | 0.79–0.99 | 0.028 |
| Fev1%pred | 0.97 | 0.96–0.99 | 0.001 | 0.97 | 0.95–1.00 | 0.017 |
Data for estimated odds ratio (OR) and 95% confidence interval (95% CIs) of the explanatory variables for poor outcome. Factors showing an association in the univariate analyses (p<0.20) were incorporated in the multivariable model. Final variable selection was performed using backward stepwise selection method (pin<0.05, pout>0.10). Single collinearity was evaluated using Pearson correlation (and multicollinearity with variance inflation factor).
In the majority of our patients, COVID-19 was not associated with a poor outcome. Survival with recovery usually occurred, even with pre-existing severe lung disease or following hospitalisation. Non-respiratory comorbidities were more strongly associated with poor outcome than genotype, baseline FEV1 or oxygen saturation, comparable to findings in usual COPD.7 Poor outcome was less likely with symptoms of anosmia or dysgeusia. Although outcome was comparable between PiZZ and PiSZ groups, mortality occurred only in PiZZ patients who also demonstrated reduction in FEV1% predicted, suggestive of accelerated disease progression. Consequently, patients with severe deficiency are advised to still employ effective avoidance strategies.
Notwithstanding the unique value of our data, we recognise the potential limitations to our study. Restricted patient access due to shielding may have introduced recruitment bias, however, this is more likely to have selected the most unwell patients and our mortality rate is unlikely to be underestimated. We did not perform an age-matched comparison with the ‘general population’. However, non-respiratory comorbidities, which are the same comorbidities that influence outcomes in the ‘general population’, were more strongly associated with a poor outcome than the level of AATD, FEV1 impairment and oxygen saturation. The evolving nature of the pandemic has introduced confounders since study commencement: vaccines and specific therapies have altered outcomes, but were only widely available following study completion. Our data therefore provides insight into the natural course of the original variant of COVID-19 in AATD patients, against which future comparisons can be made, and which provides a clinical context to indirect evidence of AATD as a risk factor.8
AATD patients remain concerned about contracting COVID-19 and continue to lead isolated lifestyles with consequences to health. Our data provides an estimate of the relative risk arising from AATD which may help guide clinicians and patients, and enable future comparisons to be made.
DisclosuresData from a preliminary analysis of the initial participants included in this cohort were presented at the European Respiratory Society Annual Congress 2021 as an e-poster presentation. The poster's abstract was published as a “Late breaking abstract” in the European Respiratory Journal 2021; 58: Suppl. 65, PA2365. https://erj.ersjournals.com/content/58/suppl_65/PA2365.
Conflicts of interestDavid Parr has received consulting fees from Mereo Biopharma, CSL Behring and Grifols, and speaker fees from CSL Behring and Grifols. Joanna Chorostowska-Wynimko has received research grants, speaker and consulting fees from Grifols, CSL Behring, CelonPharma, Pfizer, AstraZeneca, Boehringer-Ingelheim, speaker and consulting fees from Mereo Biopharma, MSD, BMS, GSK, Novartis, Roche, Chiesi, Amgen, Takeda. Angelo Corsico has nothing to disclose. Cristina Esquinas has received speaker fees from CSL Behring. Gerard N. McElvaney has received research funding from Grifols, Chiesi and PhPharma, consulting fees from Vertex, Illuma bioscience, Inhibrx and Intelia, and speakers fees from CSl Behring. Annelot D. Sark and Hanan Tanash have nothing to disclose. Maria Sucena has received speaker fees from Bial, Boehringer Ingelheim, CSL Behring and Grifols and consulting fees from Bial and CSL Behring. Alice M Turner has received research funding from CSL Behring and Vertex, consulting fees from Takeda and Inhibrx, and speaker fees from CSL Behring. Further research funding from Grifols is being contracted. Marc Miravitlles has received speaker fees from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, Menarini, Rovi, Bial, Sandoz, Zambon, CSL Behring, Grifols and Novartis, consulting fees from AstraZeneca, Atriva Therapeutics, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Bial, Gebro Pharma, CSL Behring, Laboratorios Esteve, Ferrer, Mereo Biopharma, Verona Pharma, Spin Therapeutics, ONO Pharma, pH Pharma, Palobiofarma SL, Takeda, Novartis, Sanofi and Grifols and research grants from Grifols.
FundingThis study was supported by the European Respiratory Society EARCO Clinical Research Collaboration.
Members of the IMCA1 Study Group: Robert Bals, Miriam Barrecheguren, Christian Clarenbach, Ilaria Ferrarotti, Lourdes Lazaro, José Luis Lopez-Campos, Farah Mobeen, Jan Stolk and Eva Taberno.
The authors want to thank the participants in the study and the national patients support groups that facilitated awareness of the study through their members.







