









Sexual limitations play an important role in the quality of life of patients with chronic diseases. Very limited information is available on the impact of asthma on the sexual functioning of these individuals.
Materials and methodsCross-sectional, observational, multicenter study. Asthma patients and healthy individuals were recruited. All subjects participated in an interview in which demographic and clinical data were recorded, and completed the Goldberg Anxiety-Depression Scale (GADS) to evaluate the presence of concomitant psychiatric disease. Men also completed the International Index of Erectile Function (IIEF), and women, the Female Sexual Function Index (FSFI).
ResultsA total of 276 cases were included, comprising 172 asthma patients (63 men and 109 women) with a mean age of 42 (±14) years, and 104 controls (52 men and 51 women) with a mean age of 39 (±12) years. Time since onset of asthma was 15 years and severity distribution was: 6.4% intermittent, 17.9% mild persistent, 47.4% moderate, and 28.2% severe. Disease was considered controlled in 57.7%, partially controlled in 28.2%, and uncontrolled in 14.1%. Women with asthma had greater sexual limitations than women in the control group, with a total FSFI score of 22.1 (±9) compared to 26.5 (±6.8), respectively (P<.005). Men with asthma had significantly more severe erectile dysfunction with a total IIEF score of 59.5 (±12.5) compared to 64.3 (±8.2) in male controls (P<.05). An association was also observed between sexual problems and poorer asthma control.
ConclusionsAsthma is associated with a poorer sexual quality of life among patients. These results should arouse the interest of healthcare professionals in detecting and alleviating possible sexual limitations among their asthma patients in routine clinical practice.
Las limitaciones de la vida sexual de los pacientes con enfermedades crónicas desempeñan un importante papel en su calidad de vida. La información disponible sobre el impacto de la enfermedad asmática en la vida sexual de las personas es muy limitada.
Material y métodosEstudio transversal, observacional y multicéntrico. Se reclutaron pacientes asmáticos y sujetos sanos, a los que se les efectuó una entrevista en la que se recogieron datos demográficos y clínicos y en donde además cumplimentaron los siguientes cuestionarios: la escala Goldberg Anxiety-Depression Scale (GADS) para la valoración de la existencia de comorbilidad psiquiátrica, y en varones el Índice Internacional de la Función Eréctil (IIEF) y en mujeres el Índice de la Función Sexual Femenina (FSFI).
ResultadosSe incluyeron un total de 276 casos, de los que 172 eran asmáticos (63 hombres y 109 mujeres) con una media de edad de 42 (±14) años y 104 controles (53 hombres y 51 mujeres) con una media de edad de 39 (±12) años. El asma presentaba una evolución de 15 años y su gravedad se distribuía: 6,4% intermitente, 17,9% persistente leve, 47,4% moderada y 28,2% grave. La enfermedad se consideró controlada en un 57,7%, parcialmente controlada en un 28,2% y no controlada en un 14,1%. Las mujeres asmáticas presentaron una mayor limitación de la vida sexual que las mujeres del grupo control, con una puntuación total del FSFI de 22,1 (±9) frente a 26,5 (±6,8), respectivamente (p<0,005). Y los varones asmáticos, una significativa mayor disfunción eréctil, con una puntuación total del IIFE de 59,5 (±12,5) frente a 64,3 (±8,2), respectivamente (p<0,05). Se observó además una relación entre la existencia de problemas sexuales y un peor control del asma.
ConclusionesLa enfermedad asmática condiciona una peor calidad de vida sexual en las personas afectadas. Estos resultados deberían promover, en la práctica clínica habitual, el interés de los profesionales sanitarios por determinar y paliar las posibles limitaciones sexuales de sus pacientes con asma.
There is ample evidence that sexual difficulties can accompany chronic disease.1–4 The association between sexual activity and asthma was observed some time ago, but little quantitative information is available. The notion that sex can trigger an asthma exacerbation is not implausible, and some cases have been documented. In a letter to The Lancet in 1976, the investigators Symington and Kerr found that sexual activity could induce both asthma and rhinitis.5–8 It has been reported that sexual intercourse can trigger severe asthma exacerbations requiring emergency care, hospitalization or even assisted ventilation.9,10
The physical requirements of sexual activity may cause an exacerbation of asthma, although some authors believe that emotional arousal alone is sufficient to cause or aggravate the condition. Sexercise-induced asthma,5–8 as it has been called, is for some no more than a variant of exercise-induced asthma.
However, very few studies have evaluated the sexual quality of life of patients with asthma, and the design and methodology of those that do are questionable. In a study carried out in the emergency department of the Harlem Hospital Center, New York,11 researchers asked 356 patients to assess the degree to which their asthma had adversely affected how they performed specific activities. Of these, sexual limitation was the third most frequently mentioned. Recently, Basar et al.12 found sexual dysfunction in 18 female asthma patients (47.4%) compared to four women in the control group (20%). Finally, some singular cases of erectile dysfunction (ED) in asthmatic men and the resulting impact on their sexual relations have been reported.13,14
Given these shortcomings, our objective in this study was twofold. Our first aim was to assess the potential impact of asthma on the sexual function of male and female asthma patients, and our second aim was to determine the possible factors associated with dysfunction, such as disease severity, level of control and comorbidities.
Materials and MethodsThis was an observational, cross-sectional, multicenter study conducted in a group of asthma patients of both sexes, 18 years of age and older, selected consecutively in the outpatient clinics of seven Spanish tertiary hospitals. The study was performed after approval was obtained from the respective local ethics committees. All patients were asked for written consent before participation.
Asthma was diagnosed according to GEMA criteria,15 on the basis of corresponding clinical criteria and reversible airflow obstruction documented in at least one previous lung function study. Disease severity and degree of control were also evaluated according to GEMA criteria.15 Data were collected on smoking, time since onset of asthma, possible exercise-induced asthma, pre-existing morbidity (exacerbations and hospitalizations in the year prior to inclusion), spirometry, comorbidities (allergic rhinitis, nasal polyposis, reflux, fibromyalgia, anxiety, depression, high blood pressure, diabetes), and maintenance therapy. Rhinitis was classified by severity according to the ARIA guidelines.16 All patients had stable asthma at the time of inclusion, defined as no exacerbations in the four weeks prior to inclusion.
A control group of healthy volunteers was selected from among the visitors or companions of the patients in the same outpatient clinics at the participating centers. The group selected was of a similar age to the asthma group and had no chronic respiratory diseases nor significant comorbidities.
Both groups were asked if they were concerned about their sex life, and if so, for what reasons.
Study Procedures- (a)
Psychological status was evaluated using the Goldberg Anxiety-Depression Scale (GADS).17 The GADS questionnaire asks respondents how they have felt in the past month in terms of 9 anxiety and depression items, answered dichotomously: “yes” or “no”.
- (b)
Sexuality in women was evaluated using the Female Sexual Function Index (FSFI), described by Rosen et al.18 FSFI is a self-administered questionnaire. The patient has to answer 19 different questions and select one of the six possible answers for each item that best describes their situation during the last four weeks (a score of 0 indicates that there has been no sexual activity, 1 indicates the highest functional impairment, and 5 the least functional impairment). Six different domains explored by the questionnaire are extracted from the factor analysis: “desire” (items 1 and 2); “arousal” (items 3, 4, 5, 6); “lubrication” (items 7, 8, 9, 10); “orgasm” (items 11, 12, 13); “satisfaction” (items 14, 15, 16), and “pain” (items 17, 18, 19). The total score of the assessment is the sum of all the points obtained in each domain multiplied by a factor, with a maximum score of 36. A score of less than 27 points is considered indicative of some degree of dysfunction.19
The Spanish version of the International Index of Erectile Function (IIEF) questionnaire was used in men.19,20 This is a brief, simple instrument, validated for measuring certain aspects of male sexual function. It consists of 15 items that assess different aspects of sexual function. For each question, there are several answers (range 0–5), 0 indicating the absence of sexual activity or inability to achieve intercourse. These items can be grouped into five dimensions or domains: “erectile function” (questions 1–5 and 15; score: 1–30); “orgasmic function” (questions 9 and 10; score: 2–10); “sexual desire” (questions 11 and 12; score: 2–10); “intercourse satisfaction” (questions 6–8; score: 0–15) and “overall satisfaction” (questions 13 and 14; score: 2–10). The questionnaire also has an overall score that is obtained by adding the score of all items to obtain a total ranging between 5 and 75. A score of 60 or lower is considered indicative of some degree of dysfunction.19 The IIEF can be used not only to identify possible ED, but also to stratify it according to the scores obtained on the erectile function domain21: absence of ED (a score equal to or greater than 26), mild ED (score: 17–25), moderate ED (score: 11–16) and severe ED (score: 6–10).
- (c)
Spirometry was performed according to the procedure described in the SEPAR spirometry guidelines,22 using reference values for a Mediterranean population.23
All analyses were performed using version 23.0 of the SPSS statistical package (Chicago, Illinois). A descriptive analysis was made of all variables collected from the study population. Results were expressed as percentages, frequency, and number of observations for qualitative variables, and as means with standard deviation for quantitative variables. Overall and secondary qualifications of the sexual function status of patients and controls were calculated by comparing means with the Mann–Whitney U test. Inter-group comparisons were performed using the χ2 test for categorical variables and the Kruskal–Wallis test for non-normally distributed ordinal or quantitative variables. Correlations between the score on the sexual function questionnaire and the different variables analyzed were tested using the Pearson coefficient for quantitative variables and the Spearman test for qualitative variables.
Bivariate and multivariate analyses were performed to assess the association between the different factors. Regression models were run using the factors that were associated with the dependent variable in the bivariate analysis (P<.25). Odds ratio (OR) and confidence intervals (CI) were calculated to measure the association between the variables. The presence/absence of sexual dysfunction was included as a dependent variable in both men and women separately. To facilitate the analysis, categories were pooled (IIEF greater or less than 60, and FSFI greater or less than 27). For the multivariate analysis, different models were evaluated and the most explanatory model was selected. The manual introduction method was used. Goodness-of-fit was evaluated using the Hosmer and Lemeshow test.
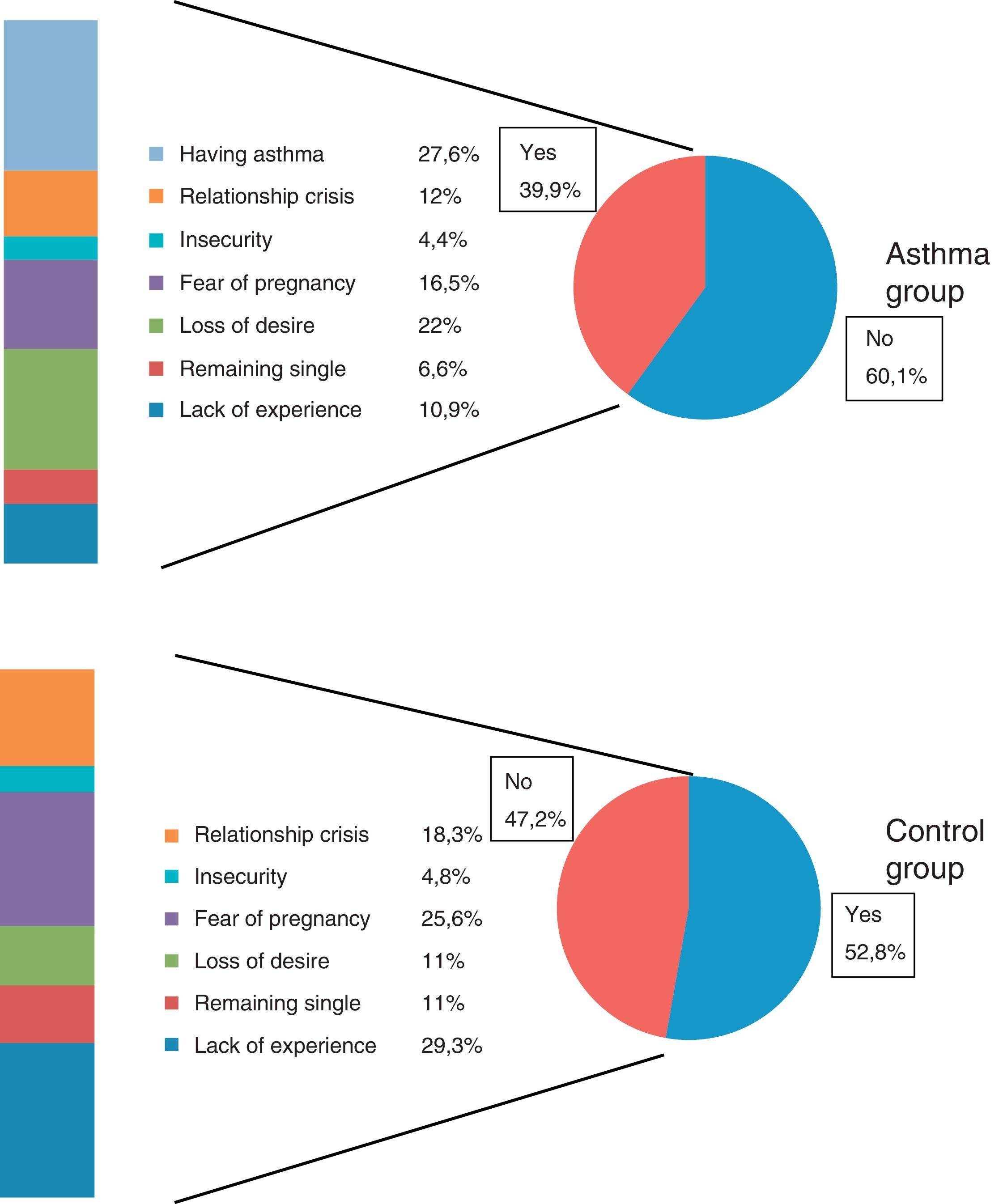
ResultsIn total, 276 cases were included, of which 172 were asthma patients (109 men and 63 women). The demographic characteristics of the study population and the clinical characteristics of asthma are reflected in Tables 1 and 2. It is interesting to note that the group of asthma patients had a significantly higher body mass index (BMI) than the control group, the percentage of smokers was similar, and asthma patients’ GADS scores were higher, both overall and in the anxiety domain. A higher proportion of men presented controlled asthma compared to women. The most common treatment for asthma was the combination of inhaled corticosteroids and long-acting beta-2 adrenoceptor agonists (LABA) (78.6%). The most significant comorbidities among the asthma group were rhinitis (80.8%), gastroesophageal reflux (20.3%), anxiety (16.8%), nasal polyposis (14.6%), depression (11.1%), arterial hypertension (11%), diabetes (4.7%), and fibromyalgia (2.9%). Concern about sexual function was expressed by 47.2% of the healthy volunteers and by 39.9% of the asthma group. Reasons for concern are listed in Fig. 1. Almost a quarter of the asthma patients associated their sexual problems with the fact of having asthma.
Comparison Between Asthma and Control Groups.
| Total (Control) | Women (Control) | Men (Control) | Total (Asthma) | Women (Asthma) | Men (Asthma) | |
|---|---|---|---|---|---|---|
| Mean age (SD) (years) | 39±12 | 39±13 | 38±10 | 42±14 | 42±15 | 42±14 |
| BMIamean (SD) | 23.9±3.6c | 22.9±3.8 | 24.9±3 | 26.5±4.6 | 26.5±5b | 27.1±4a |
| Tobacco use (%) | ||||||
| Never smoker | 61.4 | 67.4 | 54.8 | 58.1 | 66.9 | 45.9 |
| Smoker | 21.6 | 21.7 | 21.4 | 22.8 | 18.9 | 29.5 |
| Former smoker | 17 | 10.9 | 23.8 | 19.2 | 14.2 | 24.6 |
| Pack-year index (PYI) | 8±4c | 5±2 | 11±4 | 16±13 | 14±10b | 19±15a |
| GADSatotal | 3.5±4c | 4.8±4.3 | 2.3±3.3 | 6.6±4.6 | 6.8±4.6b | 6.3±4.5a |
| GADSaanxiety | 2.5±2.5c | 3.5±2.7 | 1.6±2.03 | 4.2±2.8 | 4.2±2.9b | 4.2±2.7a |
| GADSadepression | 1.8±1.9 | 1.4±2.2 | 0.68±1.6 | 2.5±2.4 | 2.6±2.4b | 2.1±2.3a |
Comparison between groups using the ANOVA test or Kruskal–Wallis for non-normally distributed variables.
BMI: body mass index; GADS: Goldberg Anxiety-Depression Scale; PYI: number of cigarettes per day×years smoking/20; SD: standard deviation.
Clinical Characteristics of Asthma Patients.
| Variable | Women (n=109) | Men (n=63) | Total (n=172) | P* |
|---|---|---|---|---|
| Admissions for asthma | ||||
| Patients admitted, n (%) | 13 (11) | 6 (7.9) | 19 (11.8) | NS |
| Admissions per patient, mean (SD) | 1.33±0.65 | 1.4±0.89 | 1.3±0.7 | |
| Emergency room visits (previous year), n (%) | 33 (30.8) | 17 (27.4) | 50 (29.6) | NS |
| Exercise-induced asthma, % | 19.4 | 28.3 | 22.7 | NS |
| Years since onset of asthma (years) | 16±11 | 15±11 | 15±11 | NS |
| Asthma control (GINA), % | ||||
| Controlled | 45.3 | 60.7 | 51.2 | .026 |
| Partially controlled | 29.2 | 18.0 | 25.0 | |
| Uncontrolled | 25.5 | 21.3 | 23.8 | |
| Asthma severity (GINA), % | ||||
| Intermittent | 8.5 | 8.2 | 8.9 | .053 |
| Persistent mild | 11.3 | 22.9 | 15.5 | |
| Persistent moderate | 43.4 | 44.3 | 43.5 | |
| Persistent severe | 36.8 | 24.6 | 32.1 | |
| Spirometry, mean (SD) | ||||
| FEV1 ml | 2.558±748 | 3.504±1.042 | 2.925±991 | NS |
| FEV1% | 85.5±22.7 | 89.4±22.4 | 87±22 | |
| FEV1/FVC, % | 72.6±12.7 | 70.8±12.7 | 72±12.7 | |
Values represent mean (standard deviation) or number of cases (percentage).
Comparisons between groups using the ANOVA test or Kruskal–Wallis for a non-normal distribution.
GINA: Global Strategy for Asthma Management and Prevention; NS: not significant; SD: standard deviation.
Differences in sexual function observed between asthma patients and controls are shown in Tables 3 and 4. Among women with asthma, overall dysfunction was significant, both in the total score and in the different dimensions of the FSFI. A significantly worse overall score was also observed in the IIEF questionnaire in men, the most affected dimensions being desire and overall satisfaction. Although there were no significant differences in the score for erectile difficulties between the group of asthma patients and the control group, according to the erectile function score only 56% of asthmatic patients reported no impotence problems compared to 74.3% in the control group. In total, 36% of asthma patients had mild ED, 4% moderate ED, and 4% severe ED.
Female Sexual Function Index (FSFI) Score in the Female Study Population.
| Variable | Asthma Group (n=109) | Control Group (n=51) | P |
|---|---|---|---|
| Overall score | 22.14±9.47 | 26.57±6.84 | <.005 |
| Arousal | 3.65±1.59 | 4.31±1.30 | <.05 |
| Desire | 3.19±1.24 | 3.8±0.97 | <.01 |
| Orgasm | 3.99±1.93 | 4.67±1.46 | <.05 |
| Pain | 3.63±1.67 | 4.16±1.23 | .070 |
| Lubrication | 4.07±1.89 | 4.77±1.41 | <.05 |
| Satisfaction | 4.25±0.17 | 4.85±0.18 | <.05 |
Data are presented as mean±standard deviation.
International Index of Erectile Function Questionnaire (IIEF) Scores in the Male Study Population.
| Variable | Asthma Group (n=63) | Control Group (n=53) | P |
|---|---|---|---|
| Overall score | 59.50±12.57 | 64.33±8.28 | <.05 |
| Erectile function | 25.97±5.82 | 27.49±4.05 | .123 |
| Sexual desire | 6.12±2.04 | 7.38±0.31 | <.005 |
| Orgasmic function | 8.93±2.13 | 9.57±1.11 | .085 |
| Satisfaction with intercourse | 11.20±3.36 | 12.15±1.80 | .278 |
| Overall satisfaction | 7.32±2.16 | 8.02±2.06 | .058 |
Data are presented as mean±standard deviation.
Among women with asthma, significant correlations were observed between the overall FSFI score and the following variables: age (−0.37; P<.001), BMI (−0.23; P=.03), time since onset of the disease (−0.36; P<.001), FEV1% (0.23; P=.02), severity and control of asthma (−0.21 and −0.27; P<.05), and emotional aspects, such as the prior existence of depression or anxiety (−0.32 and 0.26; P<.01), GADS questionnaire score (−0.32; P=.001), and previous arterial hypertension or diabetes (−0.33 and −0.32; P=.001). In men, significant correlations were found between the IIEF score and the following variables: age (−0.53; P<.0001), asthma severity (−0.41; P=.001), impaired lung function (0.39; P=.005), smoking (−0.38; P=.003), upper airway involvement (perennial rhinitis; −0.28; P=.04). In neither group, men nor women, did a previous diagnosis of exercise-induced asthma appear to be associated with sexual dysfunction.
Tables 5 and 6 show the results of the bivariate and multivariate analyses for the dysfunction/no dysfunction variable, according to the factors that might affect patients with asthma, in men and women separately. Table 5b shows the results obtained in the multivariate analysis in men which revealed an association between dysfunction and age. No associations were found for the remaining variables, although the data approached significance for degree of asthma control (P=.006). In women (Table 6b), variables that were significant in the bivariate model and age were included in the multivariate model, but no association was demonstrated, although data for degree of asthma control approached significance.
Analysis of Sexual Dysfunction in Men with Asthma.
| Variables | a. Bivariate Analysis | b. Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| Sexual Dysfunction | P | Variables | Coefficient β | OR (95% CI) | P | |||
| Yes IIEF<60 (n=24) | No IIEF>60 (n=37) | Total (n=63) | ||||||
| Smoking habit, n (%) | .10 | Age | 0.08 | 1.08 (1.02–1.15) | .005 | |||
| Never smoker/former smoker | 18 (82) | 22 (61) | 40 | |||||
| Smoker | 4 (18) | 14 (39) | 18 | |||||
| Asthma severity, n (%) | .09 | Smoking habit | −0.95 | 0.39 (0.08–1.91) | .24 | |||
| Mild/intermittent | 3 (14) | 11 (34) | 14 | Never smoker/former smoker | ||||
| Persistent-mod/severe | 18 (86) | 21 (65) | 39 | Smoker | ||||
| Degree of asthma control, n (%) | .10 | Asthma severity, n (%) | 0.63 | 1.88 (0.35–10.04) | .46 | |||
| Controlled | 15 (68) | 32 (87) | 47 | Mild/intermittent | ||||
| Uncontrolled | 7 (32) | 5 (13) | 12 | Persistent-mod/severe | ||||
| Rhinitis, n (%) | .50 | Degree of asthma control | 1.64 | 5.15 (0.91–29.18) | .06 | |||
| No | 4 (17) | 5 (13) | 9 | Controlled | ||||
| Yes | 20 (83) | 32 (86) | 52 | Uncontrolled | ||||
| Rhinitis severity, n (%) | .38 | |||||||
| Mild | 7 (37) | 17 (53) | 24 | |||||
| Moderate/severe | 12 (63) | 15 (47) | 27 | |||||
| Anxiety, n (%) | .66 | |||||||
| No | 22 (92) | 33 (92) | 56 | |||||
| Yes | 2 (8) | 3 (8) | 5 | |||||
| Depression, n (%) | 1 | |||||||
| No | 23 (96) | 35 (95) | 58 | |||||
| Yes | 2 (6) | 1 (4) | 3 | |||||
IIEF: International Index of Erectile Function Questionnaire.
Analysis of Sexual Dysfunction in Women with Asthma.
| Variables | a. Bivariate Analysis | b. Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| Sexual Dysfunction | P | Variables | Coefficient β | OR (95% CI) | P | |||
| Yes FSFI<27 (n=81) | No FSFI≥27 (n=23) | Total (n=109) | ||||||
| Smoking habit, n (%) | .11 | Age | 0.024 | 1.03 (0.99–1.07) | .18 | |||
| Never smoker/former smoker | 68 (86) | 15 (71) | 83 | |||||
| Smoker | 11 (14) | 6 (29) | 17 | |||||
| Asthma severity, n (%) | 1 | Smoking habit | −0.65 | 0.52 (0.14–1.90) | .32 | |||
| Mild-intermittent | 9 (12) | 2 (11) | 11 | Never smoker/former smoker | ||||
| Persistent-mod/severe | 66 (88) | 16 (89) | 82 | Smoker | ||||
| Degree of asthma control, n (%) | .03 | Asthma severity | −0.53 | 0.59 (0.11–3.22) | .54 | |||
| Controlled | 55 (69) | 20 (91) | 75 | Mild-intermittent | ||||
| Uncontrolled | 25 (31) | 2 (9) | 27 | Persistent-mod/severe | ||||
| Rhinitis, n (%) | .57 | Asthma control | 1.35 | 3.8 (0.82–18.22) | .08 | |||
| No | 17 (21) | 6 (27) | 23 | Controlled | ||||
| Yes | 63 (78) | 16 (73) | 80 | Uncontrolled | ||||
| Rhinitis severity, n (%) | 1 | |||||||
| Mild | 16 (25) | 4 (25) | 20 | |||||
| Moderate-severe | 47 (75) | 12 (75) | 59 | |||||
| Anxiety, n (%) | .39 | |||||||
| No | 60 (75) | 19 (86) | 80 | |||||
| Yes | 20 (25) | 3 (14) | 23 | |||||
| Depression, n (%) | .18 | |||||||
| No | 65 (81) | 21 (95) | 86 | |||||
| Yes | 15 (19) | 1 (5) | 16 | |||||
FSFI: Female Sexual Function Index.
The main finding of this study is that sexual dysfunction may be more common in both male and female patients with asthma than in the healthy population. Uncontrolled disease is probably among the factors that contribute most to this dysfunction.
Some earlier publications have reported singular cases of asthma associated with ED in men,13,14 with the consequent impact on sexual relations. ED can be defined as the persistent inability to achieve and maintain an adequate erection to allow satisfactory sexual activity. It was reported recently that asthma may be an independent risk factor for developing ED, and the more severe the bronchial disease, the closer the association.24 In our study, no significant differences were observed in the erectile function domain between asthma patients and healthy volunteers, although there was a decrease in other aspects such as sexual desire and overall satisfaction with intercourse in the group with respiratory disease. However, we found that 44% of asthma patients experienced ED, compared to only 25.7% of the control group, and that ED was more intense in the patient group. Age and uncontrolled asthma were also associated with a lower score on male sexual function scales in the multivariate analysis. Our male patients presented a better level of asthma control, and this may have led to some extent to the lack of significant impact observed in some areas of the sexual function questionnaire.
Our study corroborates the findings of recent articles that emphasize the importance of asthma in patients’ sex lives, particularly among women. Meyer et al.11 performed a study in the emergency department of a hospital in New York in which researchers asked patients attending the emergency room to assess the degree to which their asthma had adversely affected how they performed specific activities. Of these, sexual limitations were the third most frequently mentioned by the patients after climbing stairs or performing habitual household chores. Two-thirds of the patients interviewed reported sexual limitations that they associated with their asthma. These were more prevalent in patients with moderate or severe asthma compared to those with mild asthma, and in individuals over 40 years of age compared to those under the age of 40. Women with asthma who attended the emergency room reported greater sexual dysfunction than men.
In a recent study12 carried out in 38 premenopausal married women with asthma compared with 20 healthy women, FSFI was used to identify differences between these groups in terms of possible sexual dysfunction. Sexual dysfunction was observed in 18 of the asthma patients (47.4%), but in only four individuals in the control group (20%). The most severe problem in asthma patients was arousal, reported as reduced by 30 patients (78.9%), followed by decreased desire (44.7%), pain during sexual intercourse (34.2%), and difficulty reaching orgasm (31.6%). However, satisfaction scores were the least affected, and were below normal in only five individuals (13.2%). A strong correlation was also noted between the FSFI score and the scales used to evaluate the psychological status of patients, suggesting that decreased arousal and libido are related to emotional and psychological factors. These results are consistent with our findings. In our larger series, we found differences in all FSFI items, including arousal, lubrication, orgasm, desire and satisfaction, and an initial association with emotional factors, for both previously diagnosed depression or anxiety and the score attained in the psychological questionnaires. However, the multivariate analysis could not subsequently establish an explanatory model of dysfunction in asthma patients.
It should be noted that a third of our patients attributed their sexual problems to their asthma, and there is a relationship between the time since asthma onset and severity, control, and deterioration of lung function. In our series, we found that the control group was more concerned about their sexuality than the asthma group. This may be because we compared a population of patients who are probably more concerned with their many uncontrolled respiratory symptoms than their sexual function, against a healthy population with no concomitant diseases to draw their attention away from possible sexual dysfunction. In our study, it should be noted, we did not take into account the socioeconomic and/or cultural level of the study population. These factors could have an influence on our patients’ sex lives and may need to be taken into consideration in future research examining this topic.
The impact of upper airway involvement on sexual function observed in our study, particularly in men (rhinitis severity), has also been documented by other authors.25,26 Smoking is another concomitant factor to be considered in men, and may be a limiting factor in our study due to the higher consumption of tobacco among our asthma patients; however, smoking was not included the multivariate analysis as a predictor for possible dysfunction in our series. In women, the existence of comorbidities such as arterial hypertension or diabetes produced a lower score in the FSFI questionnaire. The hypothesis of so-called sexercise-induced asthma was not proved in our series, as no relationship was established between the sexual function of our patients and a previous diagnosis of exercise-induced asthma. Finally, the multivariate logistic regression seems to indicate that uncontrolled disease could be a determining factor in sexual dysfunction.
In short, sexuality is a central aspect of the quality of life of men and women and is a reflection of their level of physical, psychological and social well-being, but this issue is very often ignored in routine clinical practice. Our study found that both women and men with asthma have significant sexual dysfunction. The cause of this dysfunction is multifactorial, and several parameters appear to be involved, including the severity of symptoms and the existence of comorbidities typical of asthma, such as rhinitis and psychological dysfunction. Improving asthma control should improve not only sexual function but also other aspects of the patient's life. There is a need, however, for new studies to confirm this conclusion, and specific recommendations should be developed for patients with asthma that include aspects related to sexuality.
FundingThe project was funded by a non-restrictive grant from Novartis Farmacéutica, S.A., Spain.
Conflict of InterestJ. Gregorio Soto Campos has received fees in the past two years for speaking engagements in congresses and financial support for attending scientific events from Boehringer, Novartis, Chiesi, Astra, and GSK; Vicente Plaza has received fees in the past three years for participating as a speaker in meetings sponsored by Chiesi, Esteve, GSK, Novartis, Orion and Pfizer and as a consultant for ALK, MundiPharma, Orion and Teva. He has received financial support for attending congresses from AZ, Chiesi and Novartis and research grants from AZ, Chiesi and Menarini.
Please cite this article as: Soto Campos JG, Rojas Villegas J, Padilla Galo A, Marina Malanda N, Garcia Rivero JL, Pinedo Sierra C, et al. Impacto del asma en la vida sexual de los pacientes. Un estudio de casos y controles. Arch Bronconeumol. 2017;53:667–674.







