
Higher morbidity caused by smoking-related diseases could increase health costs. We analyzed differences in the use of healthcare resources, healthcare costs and days of work absenteeism among smokers and non-smokers.
MethodsCross-sectional study in smokers and non-smokers, aged between 45 and 74 years, from one urban health area. The variables studied were age, sex, alcohol intake, physical activity, obesity, diseases, attendance at primary care clinics and hospital emergency rooms, days of hospitalization, prescription drug consumption and work absenteeism (in days). Annual cost according to the unit cost of each service (direct costs), and indirect costs according to the number of days missed from work was calculated. Crude and adjusted risks were calculated using logistic regression.
ResultsFive hundred patients were included: 50% were smokers, 74% (372) men and 26% (128) women. Smokers used more healthcare resources, consumed more prescription drugs and had more days off work than non-smokers. Respective direct and indirect costs in smokers were 848.64 euros (IQ 25–75: 332.65–1517.10) and 2253.90 euros (IQ 25–75: 1024.50–13113.60), and in non-smokers were 474.71 euros (IQ 25–75: 172.88–979.59) and 1434.30 euros (IQ 25–75: 614.70–4712.70). The likelihood of generating high healthcare costs was more than double for smokers (OR=2.14; 95% CI: 1.44–3.19).
ConclusionMore investment in programs for the prevention and treatment of smoking, as a health policy priority, could help to reduce the health and social costs of smoking.
La mayor morbilidad ocasionada por el tabaquismo puede generar un incremento del coste sanitario. Analizamos la existencia de diferencias en el uso de recursos sanitarios, gasto sanitario y bajas laborales entre pacientes fumadores y no fumadores.
MétodosEstudio observacional transversal en pacientes fumadores y no fumadores de edad entre 45 y 74 años atendidos en una zona de salud urbana. Variables estudiadas: edad, sexo, consumo de alcohol, actividad física, obesidad, presencia de enfermedades, frecuentación a las consultas de atención primaria e interconsultas, asistencia a urgencias hospitalarias, días de hospitalización, consumo de fármacos y días de baja laboral. Se calculó el coste anual según el coste unitario de cada servicio (costes directos) y los costes indirectos según el número de días de baja. Se calcularon los riesgos crudos y ajustados mediante regresión logística.
ResultadosSe analizaron 500 pacientes, el 50% fueron fumadores; 74% (372) hombres, 26% (128) mujeres. Los pacientes fumadores utilizaron más recursos sanitarios, consumieron más fármacos y tuvieron más días de baja laboral que los no fumadores. Los costes directos e indirectos en fumadores fueron respectivamente 848,64 euros (IQ 25-75: 332,65-1517,10) y 2.253,90 (IQ 25-75: 1.024,50-13.113,60); y en no fumadores 474,71 euros (IQ 25-75: 172,88-979,59) y 1.434,30 euros (IQ 25-75: 614,70-4.712,70); ser fumador incrementó más del doble la probabilidad de tener coste sanitario elevado (OR=2,14; IC 95%: 1,44-3,19).
ConclusiónInvertir más recursos en la prevención y el tratamiento del tabaquismo como una prioridad de política sanitaria contribuiría a la reducción en el medio plazo del sobrecoste que supone el consumo de tabaco.
The pernicious effects of smoking on health and its enormous social and economic burden are well-known and have been confirmed in numerous studies.1 Smoking may have a serious impact on national economies. The World Bank calculated that high-income countries presently allocate between 6% and 15% of their total healthcare budget to the treatment of smoking-related diseases, estimating an annual financial loss of $200bn due to the cost of healthcare and loss of productivity in smokers.2
Smoking causes cardiovascular, cerebrovascular, and respiratory diseases, as well as various cancers. Smokers are more inclined to develop a greater range of diseases, they have poorer health than non-smokers, and are more susceptible to upper respiratory tract infections and influenza.3 One consequence of this is higher work absenteeism. Smoking also affects passive smokers who inhale second-hand smoke. The economic burden of passive smoking is difficult to estimate, but it can increase the costs of smoking by around 15%, depending on the regulatory measures adopted in each country.4 The United States Department of Health periodically issues a report on the health consequences of smoking, in which they cite various U.S. studies that have demonstrated higher consumption of healthcare resources and higher rates of work absenteeism among smokers.5 Studies conducted in many other countries also reveal higher work absenteeism with more frequent and longer periods of sick leave per year in smokers compared with non-smokers.6
In former smokers, work productivity rises by 4.5% within 1 year after stopping smoking, compared with workers who continued to smoke; productivity continues to rise over time until it reaches the same levels as in non-smoking employees.7 When studying the benefits of smoking cessation in adults, researchers must take into account the length of abstinence, since many smokers stop smoking when they fall ill, which may bias the study of trends in health costs after cessation. Kahende reported that within less than 3 years after cessation, former smokers had 46% higher hospitalization costs, while this figure fell to 22% between 3 and 15 years after cessation; after 15 years, hospitalization costs were similar to those of never-smokers.8 Wagner also found that former smokers generate more healthcare costs than non-smokers in the first 4 years after cessation.9 Accordingly, the use of retrospective studies to classify the health cost generated by this heterogeneous group may be problematic.
Direct healthcare services deriving from the 5 main smoking-related diseases cost €7695.29 million in Spain in 2009. Furthermore, in that year, indirect costs of smoking on the work environment amounted to €8.78bn. This figure includes work absenteeism due to smoking-related illness, loss of productivity, and maintenance and cleaning of facilities.10
According to the latest data, 24% of Spaniards older than 15 years of age are smokers.11 Various studies underline the relationship between the modification of risk factors and healthcare costs in the short term in several countries, but no detailed study has been conducted in the general population in our country. The aim of this study was to examine any significant difference in the use of healthcare resources, healthcare spending, and sick leave between smokers and non-smokers seen in an urban healthcare district.
Materials and MethodsThis was a cross-sectional observational study in patients seen in the consultation rooms of 14 primary care physicians in a standard urban healthcare district. The patient population was selected by convenience sampling from among patients with a complete electronic medical history for 2009, attended at the primary care level between 2010 and 2011. Recruitment was based on quotas for age, sex, and expected prevalence of smoking among 3 age groups (45–54; 55–64 and 65–74 years). For inclusion, patients had to be a public health system user with an active clinical record between January and December 2009, aged between 45 and 74 years. A smoker was defined as a subject who had smoked daily during the year of the study, and a non-smoker was one who had not smoked regularly at any time during their life; former smokers were excluded.
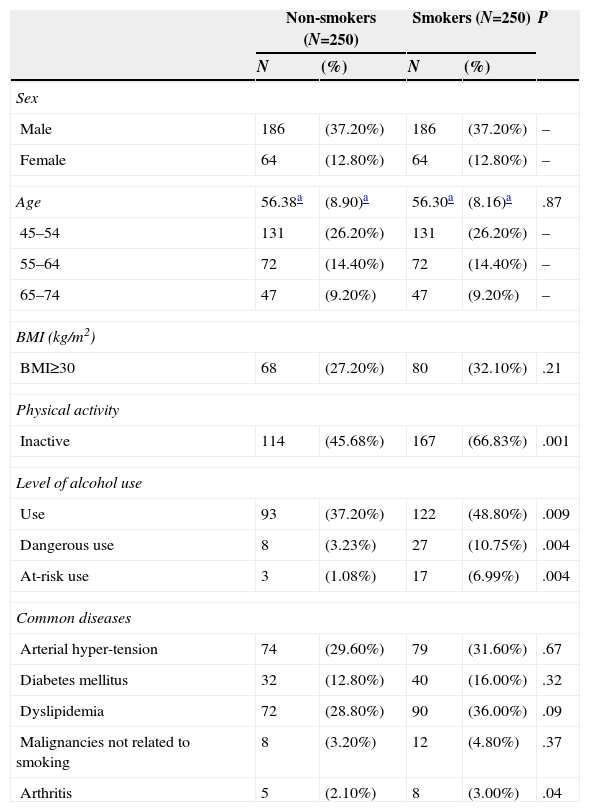
Study variables included: age, sex, alcohol use (at-risk consumption was considered 28units/week ≥ in men and ≥17units/week in women; dangerous consumption was 17–28units/week in men and 11–17units/week in women), physical activity (a subject was considered active if they did more than 20min of aerobic activity at least 3 days a week), obesity (body mass index [BMI]≥30kg/m2) and presence of prevalent diseases (arterial hypertension, diabetes mellitus, dyslipidemia, malignancies, and arthritis). Variables related to the use of healthcare services were frequency of visits to primary health care consultations (with a doctor or a nurse), number of days of hospitalization throughout the year, and drug prescription records. Chronic prescription was considered any chronic use of medications (daily, weekly or monthly) at the time of the study. Number of days off work for temporary sick leave was recorded for each patient; these data were collected only for patients who were actively employed. All study data were retrieved from the patients’ electronic clinical records.
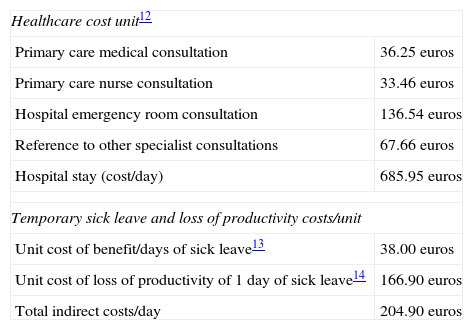
Economic estimates of direct costs were calculated from data provided by the regional health department.12 The annual cost was determined by multiplying the unit cost by the number of consultations or days of hospital stay in each of the study categories. Unit costs per process are given in Table 1. To evaluate the indirect costs related to loss of productivity, the unit cost was multiplied by the number of days of sick leave. The costs of sick leave benefits were calculated from the first day of leave, according to applicable legislation,13 and added to the cost of lost productivity estimated by the CEOE (Spanish Confederation of Employers’ Organizations)14 (Table 1).
Unit Costs of Healthcare Services and Temporary Sick Leave and Loss of Productivity.
| Healthcare cost unit12 | |
| Primary care medical consultation | 36.25euros |
| Primary care nurse consultation | 33.46euros |
| Hospital emergency room consultation | 136.54euros |
| Reference to other specialist consultations | 67.66euros |
| Hospital stay (cost/day) | 685.95euros |
| Temporary sick leave and loss of productivity costs/unit | |
| Unit cost of benefit/days of sick leave13 | 38.00euros |
| Unit cost of loss of productivity of 1 day of sick leave14 | 166.90euros |
| Total indirect costs/day | 204.90euros |
The sample size was calculated for a two-tailed comparison of means, a 95% confidence interval, a statistical power of 80%, 15% precision and an expected variance of 3006. The result was a minimum of 210 subjects per group.
Quantitative variables were described using means and standard deviations if distribution was normal, and medians and interquartile ranges (Q1–Q3) in all other cases. Qualitative variables were described using absolute frequencies and percentages. The 95% confidence interval was calculated for all variables; if this was unsuitable, the interquartile range was provided. Goodness of fit to the normal distribution was evaluated by the Kolmogorov–Smirnov test. For variables that did not adjust to the normal distribution we used non-parametric tests to compare 2 independent samples (Mann–Whitney U test) and the Kruskal–Wallis H test (for more than 2 samples). For variables that did adjust to the normal distribution, the ANOVA and Student's t-test were used. The association between qualitative variables was explored using hypothesis testing techniques for the comparison of proportions (Chi-squared, Fisher's exact test). For all comparisons, the level of significance was set at 5%. In the multivariate analysis, a high-cost individual was used as a dependent variable, defined as a public system user with an average cost higher than that of the mean of the overall population. Independent variables included: age, sex, smoking, alcohol use, physical activity, BMI, and the presence of the prevalent diseases listed above. Crude risks were calculated using bivariate logistic regression models. To calculate adjusted risks, a multivariate logistic regression model was performed using the stepwise procedure. The software package Stata 9.1 was used for the statistical analysis.
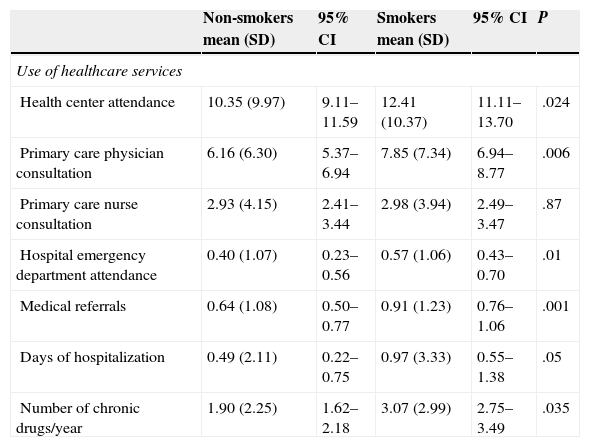
ResultsIn total, 500 patients aged between 45 and 74 years were included in the study. Of these, 74% (372) were men and 26% (128) were women; 50% were smokers and the other 50% had never smoked. The characteristics of the study population are described in Table 2. Smokers consumed more alcohol and did less physical activity than non-smokers. The use of healthcare resources, annual use of chronic drugs, and days of sick leave in smokers and non-smokers are listed in Table 3. Except for nurse consultations, the smokers used all healthcare resources more frequently than non-smokers, spent more days in hospital, used more chronic prescription drugs, and took more days of sick leave. The differences were statistically significant in all cases.
Study Population Characteristics.
| Non-smokers (N=250) | Smokers (N=250) | P | |||
|---|---|---|---|---|---|
| N | (%) | N | (%) | ||
| Sex | |||||
| Male | 186 | (37.20%) | 186 | (37.20%) | – |
| Female | 64 | (12.80%) | 64 | (12.80%) | – |
| Age | 56.38a | (8.90)a | 56.30a | (8.16)a | .87 |
| 45–54 | 131 | (26.20%) | 131 | (26.20%) | – |
| 55–64 | 72 | (14.40%) | 72 | (14.40%) | – |
| 65–74 | 47 | (9.20%) | 47 | (9.20%) | – |
| BMI (kg/m2) | |||||
| BMI≥30 | 68 | (27.20%) | 80 | (32.10%) | .21 |
| Physical activity | |||||
| Inactive | 114 | (45.68%) | 167 | (66.83%) | .001 |
| Level of alcohol use | |||||
| Use | 93 | (37.20%) | 122 | (48.80%) | .009 |
| Dangerous use | 8 | (3.23%) | 27 | (10.75%) | .004 |
| At-risk use | 3 | (1.08%) | 17 | (6.99%) | .004 |
| Common diseases | |||||
| Arterial hyper-tension | 74 | (29.60%) | 79 | (31.60%) | .67 |
| Diabetes mellitus | 32 | (12.80%) | 40 | (16.00%) | .32 |
| Dyslipidemia | 72 | (28.80%) | 90 | (36.00%) | .09 |
| Malignancies not related to smoking | 8 | (3.20%) | 12 | (4.80%) | .37 |
| Arthritis | 5 | (2.10%) | 8 | (3.00%) | .04 |
Use of Healthcare Services, Chronic Drug Use, and Temporary Sick Leave in Smokers and Non-smokers.
| Non-smokers mean (SD) | 95% CI | Smokers mean (SD) | 95% CI | P | |
|---|---|---|---|---|---|
| Use of healthcare services | |||||
| Health center attendance | 10.35 (9.97) | 9.11–11.59 | 12.41 (10.37) | 11.11–13.70 | .024 |
| Primary care physician consultation | 6.16 (6.30) | 5.37–6.94 | 7.85 (7.34) | 6.94–8.77 | .006 |
| Primary care nurse consultation | 2.93 (4.15) | 2.41–3.44 | 2.98 (3.94) | 2.49–3.47 | .87 |
| Hospital emergency department attendance | 0.40 (1.07) | 0.23–0.56 | 0.57 (1.06) | 0.43–0.70 | .01 |
| Medical referrals | 0.64 (1.08) | 0.50–0.77 | 0.91 (1.23) | 0.76–1.06 | .001 |
| Days of hospitalization | 0.49 (2.11) | 0.22–0.75 | 0.97 (3.33) | 0.55–1.38 | .05 |
| Number of chronic drugs/year | 1.90 (2.25) | 1.62–2.18 | 3.07 (2.99) | 2.75–3.49 | .035 |
| Median | IQR 25–75 | Median | IQR 25–75 | P | |
|---|---|---|---|---|---|
| Temporary sick leave | |||||
| Days of temporary sick leave | 7 | 3–23 | 11 | 5–64 | .025 |
SD, standard deviation.
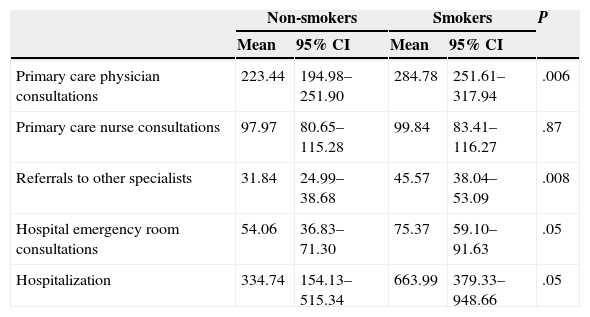
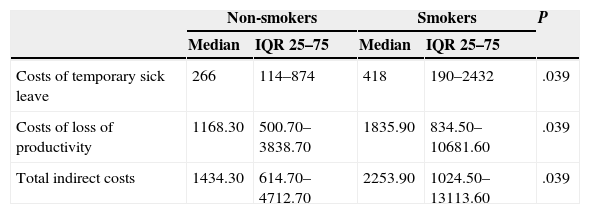
The annual costs of the different healthcare services used by smokers and non-smokers and overall health expenditure are shown in Table 4: spending was on average €474.71 for non-smokers and €848.64 for smokers. These differences were statistically significant (P=.0001). Average indirect costs in non-smokers were €1434.3, and €2253.90 in smokers (Table 5).
Annual Costs of Healthcare Services in Non-smokers and Smokers (Euros).
| Non-smokers | Smokers | P | |||
|---|---|---|---|---|---|
| Mean | 95% CI | Mean | 95% CI | ||
| Primary care physician consultations | 223.44 | 194.98–251.90 | 284.78 | 251.61–317.94 | .006 |
| Primary care nurse consultations | 97.97 | 80.65–115.28 | 99.84 | 83.41–116.27 | .87 |
| Referrals to other specialists | 31.84 | 24.99–38.68 | 45.57 | 38.04–53.09 | .008 |
| Hospital emergency room consultations | 54.06 | 36.83–71.30 | 75.37 | 59.10–91.63 | .05 |
| Hospitalization | 334.74 | 154.13–515.34 | 663.99 | 379.33–948.66 | .05 |
| Median | IQR 25–75 | Median | IQR 25–75 | ||
|---|---|---|---|---|---|
| Chronic drugs | 95.86 | 0–349.01 | 186.60 | 13.23–567.64 | .0002 |
| Overall annual healthcare expenditure | 474.71 | 172.88–979.59 | 848.64 | 332.65–1517.10 | .0001 |
Annual Indirect Costs in Non-smokers and Smokers (Euros).
| Non-smokers | Smokers | P | |||
|---|---|---|---|---|---|
| Median | IQR 25–75 | Median | IQR 25–75 | ||
| Costs of temporary sick leave | 266 | 114–874 | 418 | 190–2432 | .039 |
| Costs of loss of productivity | 1168.30 | 500.70–3838.70 | 1835.90 | 834.50–10681.60 | .039 |
| Total indirect costs | 1434.30 | 614.70–4712.70 | 2253.90 | 1024.50–13113.60 | .039 |
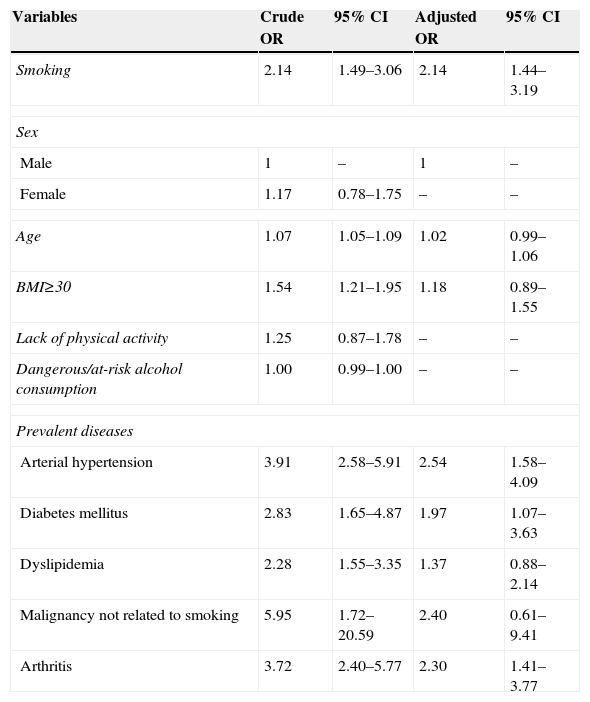
The multivariate analysis showed how the probability of generating high healthcare costs is more than doubled in smokers (OR=2.14; 95% CI: 1.44–3.19). This probability was maintained, despite adjusting for other variables that might affect health spending such as hypertension, diabetes, dyslipidemia, arthritis or cancer (Table 6).
Crude and Adjusted Risks of Increased Healthcare Costs.
| Variables | Crude OR | 95% CI | Adjusted OR | 95% CI |
|---|---|---|---|---|
| Smoking | 2.14 | 1.49–3.06 | 2.14 | 1.44–3.19 |
| Sex | ||||
| Male | 1 | – | 1 | – |
| Female | 1.17 | 0.78–1.75 | – | – |
| Age | 1.07 | 1.05–1.09 | 1.02 | 0.99–1.06 |
| BMI≥30 | 1.54 | 1.21–1.95 | 1.18 | 0.89–1.55 |
| Lack of physical activity | 1.25 | 0.87–1.78 | – | – |
| Dangerous/at-risk alcohol consumption | 1.00 | 0.99–1.00 | – | – |
| Prevalent diseases | ||||
| Arterial hypertension | 3.91 | 2.58–5.91 | 2.54 | 1.58–4.09 |
| Diabetes mellitus | 2.83 | 1.65–4.87 | 1.97 | 1.07–3.63 |
| Dyslipidemia | 2.28 | 1.55–3.35 | 1.37 | 0.88–2.14 |
| Malignancy not related to smoking | 5.95 | 1.72–20.59 | 2.40 | 0.61–9.41 |
| Arthritis | 3.72 | 2.40–5.77 | 2.30 | 1.41–3.77 |
Our results show that the annual healthcare expenditure was €848.64 for smokers and €474.71 for non-smokers, representing excess costs of 44%. Several studies have used different methods to evaluate the increased burden to the healthcare budget caused by smokers. An estimation performed in the U.S. in 2012 showed that smokers accounted for more health spending than never-smokers, calculating excess health costs for smokers according to age range. More recently, Wacker et al. conducted a study on the general use of healthcare services in Germany among 3071 individuals aged between 32 and 81 years. Data were adjusted by age, sex, education, alcohol consumption, and physical activity. Costs for non-smokers were €3237 while for smokers, they amounted to €3980, with excess costs of 18.7%.15 In our study, we included smokers aged between 45 and 74 years, since, as reported by other authors, differences in healthcare costs are the most apparent in this range.5 In general, younger subjects (<45 years) have better health, and many smokers have not been smoking long enough for the harmful effects of tobacco to have developed. In patients older than 75 years, differences in costs are also less noticeable, since surviving smokers tend to have a lower disease burden and use healthcare services to a lesser degree. Moreover, elderly individuals in general have a higher disease burden.4 Thus, we evaluated costs in the population sector with the greatest differences, and this methodological characteristic may explain why our results show greater increases than other studies. Differences in health systems between countries could also explain the differences in the magnitude of healthcare costs.
As our results indicate, the excess costs generated by smokers is directly related to greater use of healthcare services, chronic medication, and increased periods of sick leave. We studied the cost per day of hospital stay, without taking into account the reason for admission. As such, the difference in hospital costs between smokers and non-smokers may have been underestimated, since cost related with hospitalization for chronic diseases is higher than the average daily cost, and chronicity is more common in smokers. Several studies have highlighted the significant increase in hospitalization rates among adult smokers compared with never-smokers; differences as high as 30%–45% have been reported in studies with more than 5 years’ follow-up.8 Other groups have also reported a moderate increase of about 7–15% in the number of outpatient consultations.9 When we compared the use of primary care nurse consultations by smokers with non-smokers, we found similar frequency of visits and, consequently, similar costs. In contrast, other authors have reported increased use of nurse consultations by smokers ranging from 32% in individuals aged 65–74 years to 56% in the 45–65 age group.16
The multivariate analysis showed how the probability of being a high healthcare-cost individual is more than doubled in smokers (OR=2.14; 95% CI: 1.44–3.19). This risk remains unchanged after adjusting for other known high-cost variables, such as hypertension, diabetes, or dyslipidemia. It is worth noting that of all the risk factors considered, smoking was the only health determinant that is clearly modifiable with the application of cost-effective healthcare interventions.17 A recent study found that the cost of medications per smoker in a smoking cessation clinic was €118, while the cost for a smoker who had successfully stopped after 1 year was €215.18 This clearly underlines the need to prioritize smoking cessation within the public health system and to finance these initiatives as an effective method for reducing health costs, which as we have seen are considerably greater among smokers.
With regard to indirect costs, the evidence consistently shows that smoking increases both the risk and duration of work absenteeism. In our study, we found an annual cost for temporary sick leave and loss of productivity of €2593.90 in smokers and €1434.30 in non-smokers, representing a loss of €819.60 per smoker. Studies conducted in other countries have evaluated the increase in sick leave among smokers, estimating the loss of years worked. They found that the corresponding loss of productivity may account for as much as 0.74% of gross domestic product.19 The relationship between smoking and work absenteeism in the active population was recently quantified in a systematic review and meta-analysis of longitudinal and cohort studies. This study showed that smokers had a 33% greater probability of taking sick leave, and that they were absent 2.74 working days more than non-smokers6; our data were similar. This suggests that anti-smoking policies and programs need to be targeted at workers, as such measures can be expected to significantly increase work productivity and generate economic savings.
In our study, when direct costs (healthcare) and indirect costs (absenteeism, loss of productivity, etc.) were taken together, the total excess costs attributed to smoking add up to €1193.50/year (€373.90 in excess healthcare costs and €819.60 for absenteeism and loss of productivity). This coincides with the findings of other recent economic studies which, despite methodological and geographical, also found that smoking, in addition to its well-recognized health problems, drains both health and non-health resources, and has far-reaching social consequences.20–23 In contrast, investment in smoking cessation programs may be highly beneficial from an economic point of view. This was the conclusion of a study conducted in California on the costs of smoking cessation initiatives, estimated at $2.4bn, and savings in health expenditure brought about by the introduction of such measures. The authors found that each dollar spent on prevention can generate savings of $55 in terms of health costs.24 In Spain, despite the implementation of anti-smoking measures in recent years, 1 in 7 deaths a year in individuals older than 35 years is attributable to smoking, suggesting that much remains to be done.25,26
Our study has some limitations that should be pointed out. Firstly, the fact that it was conducted in a primary care setting may constitute a limitation. However, data from this setting may be more easily extrapolated to the general population, allowing for a better estimate of the overall costs of smoking. Moreover, the use of computerized clinical records coupled with access to hospital data (emergency department care, consultations and hospitalization) from this setting yielded more homogeneous information. Another possible limitation is the exclusion of former smokers. We excluded these subjects for 2 reasons: firstly, some authors have reported that smokers who have recently given up use more healthcare resources in the short term,8,9 because they have stopped smoking due to illness; and, secondly, former smokers form a very heterogeneous group, with widely varying periods since cessation. We do not believe, however, that this exclusion criterion invalidates the results obtained, since this is a subpopulation that differs from both the smoking population and the non-smoking population. Another possible limitation is the fact that we based our calculations on units costs applied in the Aragon Health System, which may not coincide with those of other autonomous communities in Spain. However, the relative difference in costs between smokers and non-smokers is likely to be similar. The main strength of our study is that it is the first microeconomic study performed in Spain that estimates the real health costs associated with smoking in a well-defined urban community.
In summary, our results underline the importance of smoking in increasing health costs, and highlight the need to establish smoking prevention and cessation measures as a healthcare policy priority that will help reduce the excess healthcare and social costs generated by lifetime smoking. Measures should include public funding of smoking cessation initiatives. These can be very effective, and although their impact on the prevalence of smoking is modest, they may contribute in the midterm to reducing the healthcare and social burden of smoking.27,28 Studies evaluating the economic costs of smoking show the benefits that can be obtained by smoking prevention and cessation programs in a community. Positive outcomes include not only a more healthy population, but also reduced healthcare spending and a more sustainable public health system.
FundingThis project was funded by the B86 Smoking Research Group, an initiative of the Government of Aragon.
Authors/Co-workersR. Córdoba-García, M.V. Villaverde-Royo, M.P. Suárez-Bonel and I. Nerín conceived the study, analyzed the data and produced the first version of the manuscript. M.P. Suárez-Bonel conducted the fieldwork, along with J. Mezquida-Arno, and C. Sanz-Andrés contributed to the Discussion section and critical review of the manuscript. The final version was evaluated and approved by all the authors before submission.
Conflict of InterestsThe authors declare that they had no conflict of interests.
We thank Natalia Enríquez of the Department of Health, Social and Family Welfare of the Government of Aragon for data on the units costs of medical services in the Community of Aragon. We also thank Ángel López-Nicolás for his critical reading of the manuscript.
Please cite this article as: Suárez-Bonel MP, Villaverde-Royo MV, Nerín I, Sanz-Andrés C, Mezquida-Arno J, Córdoba-García R. Costes derivados del uso de servicios sanitarios y bajas laborales en pacientes fumadores: estudio en una comunidad urbana. Arch Bronconeumol. 2015;51:615–620.







