



We report 2 similar cases of diagnosis by pathology study of a granulomatous reaction caused by hemostatic material (oxidized cellulose, Surgicel®) that occurred in 2019 at the Hospital Universitario Virgen de las Nieves in Granada.
The first was a 61-year-old patient with no significant medical history, diagnosed with a solitary pulmonary nodule measuring 15mm×20mm in the right inferior lobe. Right lower lobectomy was performed by video-assisted thoracoscopy (VATS) with a histological diagnosis of adenocarcinoma of pulmonary origin. Follow-up computed tomography (CT) showed right lower paratracheal nodes (station 4R) measuring 19mm×16mm, enlarged compared to previous imaging studies, so linear endobronchial ultrasound transbronchial needle aspiration (EBUS-TBNA) was performed. The pathology study of the node revealed multiple inclusions of birefringent material under polarized light, suggestive of oxidized cellulose (Surgicel®) and cells with evidence of histiocytic/macrophagic reaction to a foreign body. It was subsequently determined that during the surgical process, hemostatic material had been used near the 4R space (Fig. 1).
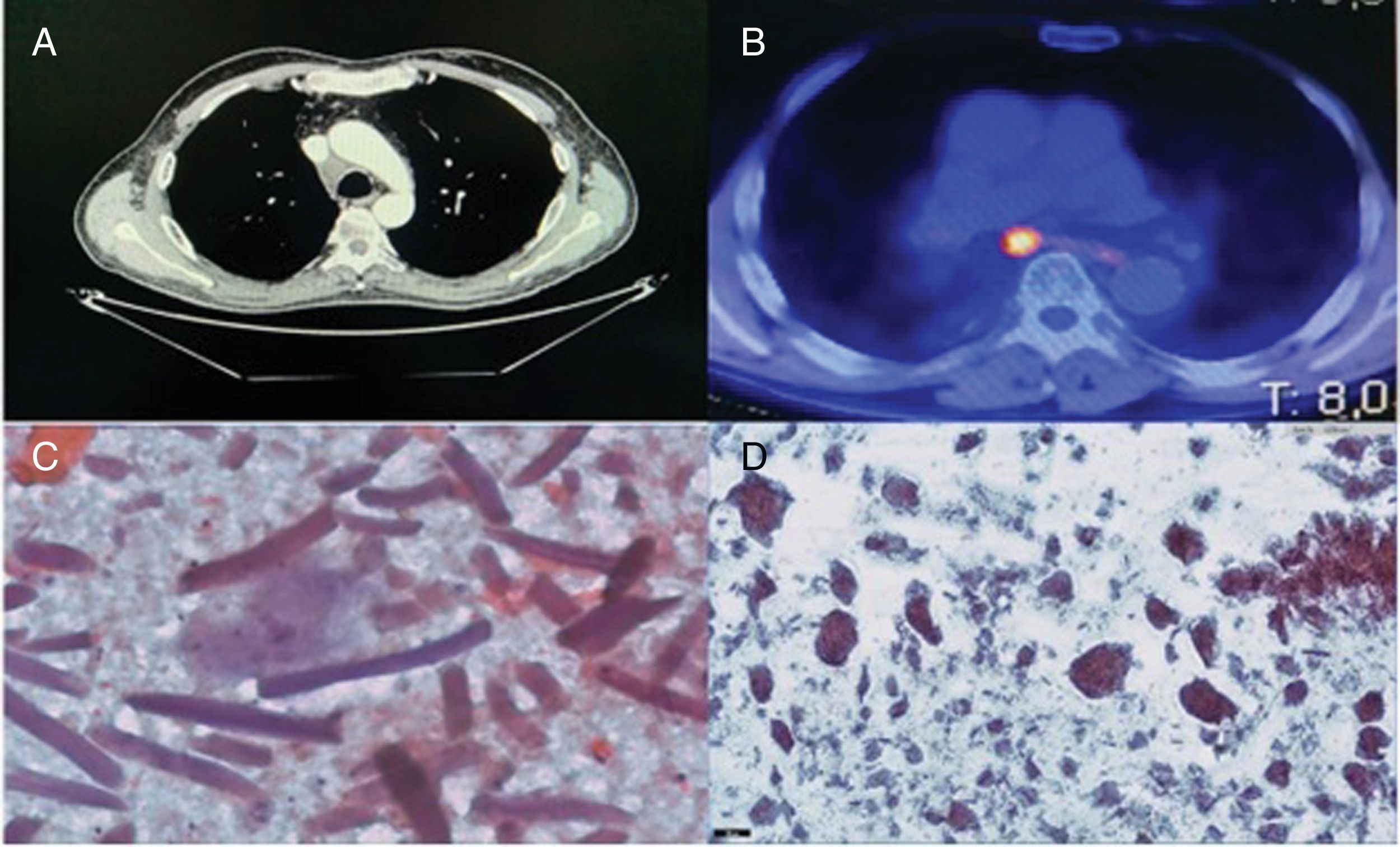
The second case was a 70-year-old man with a history of right lower lobectomy by VATS, with mediastinal lymphadenectomy at 4R and in the subcarinal region (G7) due to a pulmonary nodule measuring 22mm×14mm, with a histologic diagnosis of invasive keratinizing squamous cell carcinoma. In the follow-up CT, enlarged mediastinal nodes were observed, so positron emission tomography (PET/CT) was performed, revealing hypermetabolism at the G7 and right upper paratracheal stations (2R). Nodal neoplastic relapse was suspected, so EBUS-TBNA was performed, showing adenopathy at 2R and a rounded image measuring about 15 mm in its short axis at G7. Three aspirations were made of each lesion in the presence of a cytopathologist, and the initial diagnosis was granuloma. The definitive diagnosis was non-necrotizing giant cell granulomatous reaction and birefringent amorphous material under polarized light, with no neoplastic cells. Similarly, it was confirmed that Surgical® had been used in the adenopathic beds during surgery.
The use of Surgicel® has been widespread in virtually all surgical fields for decades, and its safety and hemostatic properties have been demonstrated, although its mechanism of action is not yet fully clarified. In the vast majority of cases, complete resorption occurs between 1 and 2 weeks after the intervention, starting as soon as 24h post-surgery. Resorption depends on the amount of Surgicel® used in the procedure and the saturation of this material by blood and the tissue bed. Cases of complications due to the excessive use of this hemostat have been documented.1 Although a greater number of cases have been reported in cardiovascular,2 maxillary,3 and abdominal surgeries, reactions of this nature have also been described in patients undergoing thoracic surgery,4 although this is the first report in the literature of 2 cases. Similar reactions have been described with the inclusion of other materials, such as sutures, talc, and implants,5 and a histological study of the lesion must be performed if a neoplastic process is suspected that cannot be ruled out by other procedures. The presence of this material must be taken into account during the differential diagnosis prior to cytohistological confirmation.
Please cite this article as: Díaz López JM, Caballero Vázquez A, López Hidalgo JL, Márquez Lobo B. Diagnóstico mediante EBUS-TBNA de reacción granulomatosa secundaria a Surgicel® en adenopatía mediastínica. Arch Bronconeumol. 2020;56:460–461.







