



Deciduoid mesothelioma is a rare variant of epithelioid mesothelioma, with a poor prognosis. It has unknown aetiology unrelated to asbestos exposure. Few cases have been reported in the literature to date. The best treatment remains a matter of debate.
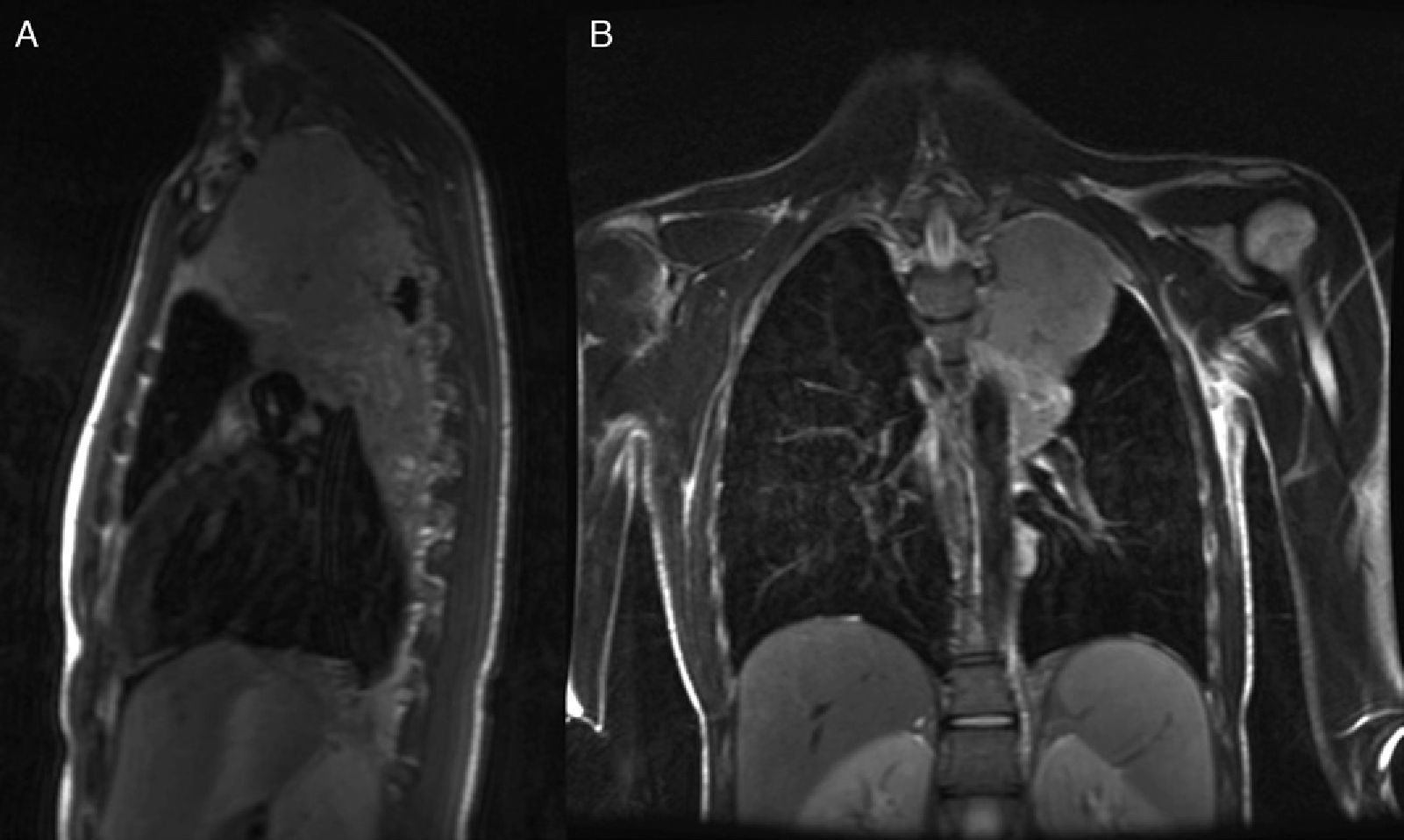
We describe an unusual case (due to the age and lack of any history) of a 17-year-old patient that began with a persistent non-productive cough but no other symptoms, and which did not improve despite antibiotic and analgesic treatment. Laboratory tests revealed hypochromic microcytic anaemia, thrombocytosis and high C-reactive protein (CRP). On the X-ray, a multilobular mass was identified that the chest computed tomography (CT) scan described as a 9cm heterogeneous solid mass in the left upper lobe. Atelectasia of the surrounding lung parenchyma was noted on magnetic resonance imaging (MRI), defining the mass as extrapulmonary and derived from the pleura; it also infiltrated the mediastinum, partially surrounding the left subclavian artery at its origin (Fig. 1). There were no endobronchial changes and bronchial aspirate (BAS) cultures were negative. The study was completed with a positron emission tomography (PET) scan, which showed hypermetabolism of the mass with maximum SUV of 8.55, and no uptake in the mediastinum.
A fine needle aspiration biopsy (FNAB) of the mass was performed, in which pathological malignant cells were obtained, followed by a diagnostic surgical biopsy. Samples of the mass were taken during the surgery, and infiltration of the mediastinum, aortic arch and aortopulmonary window was confirmed. The histopathology study found malignant large epithelial cells, with eosinophilic cytoplasm and round nuclei; the cytoplasm was positive for cytokeratin AE1/AE3, calretinin and WT-1; the nucleus was positive for epithelial membrane antigen (EMA) and negative for thyroid transcription factor 1 (TTF1). These findings were consistent with a diagnosis of deciduoid pleural mesothelioma. Clinical staging according to the International Mesothelioma Interest Group (IMIG) was T3-N0-M0 (stage III). Radical surgery (extrapleural pneumonectomy) was ruled out and chemotherapy was started with cisplatin and pemetrexed. The patient presently has a survival of 21 months.
Malignant pleural mesothelioma, the most common primary malignant pleural tumour, is a rare disease, but its incidence has been increasing in Europe. There are four main histological subtypes: epithelioid, sarcomatoid, desmoplastic and biphasic. Malignant deciduoid mesothelioma (MDM) is a very rare variant of epithelioid mesothelioma, accounting for less than 5% of mesotheliomas. First described by Talerman et al. in 1985, 23 cases of this subtype in the pleural cavity have been published to date,1 the latest by Santos et al.2 MDM generally has a poor prognosis, and 68% of patients die within the first year after commencing treatment. Aetiopathogenically, it is not related to asbestos exposure, as the early age of onset of these lesions confirms; theories refer to chromosome abnormalities of unknown significance. The role of surgery as a treatment is controversial. Debulking may sometimes be offered, which slows tumour progression and increases survival. Two techniques have been developed based on this3: extrapleural pneumonectomy and pleurectomy/decortication. Neither appears to be superior in terms of survival, but the selection of epithelial tumours without lymph node metastases for debulking surgery has demonstrated a survival benefit with respect to systemic support therapy.4 Neoadjuvant treatment is accepted as standard therapy in stage IIIA, and is being investigated as therapy in earlier stages. Byrne et al. initially published good responses to cisplatin and gemcitabine, but studies in this line later showed that the combination that provided greater survival benefit was pemetrexed with cisplatin.5 Radiotherapy has been beneficial in the prevention of recurrence after surgery, forming part of trimodal therapy. The therapeutic decision will be the one that is most beneficial in terms of survival, so determining factors for poor survival must be defined, such as6: advanced age, poor performance, non-epithelioid type, leukocytosis and high CRP. In conclusion, debulking can be offered to patients with MDM without lymph node involvement, recommending neoadjuvant treatment with cisplatin and pemetrexed in advanced stages.
Please cite this article as: Arango-Tomás E, et al. Mesotelioma deciduoide pleural en un adolescente. Arch Bronconeumol. 2013; 49:218-9.







