

Post-pneumonectomy bronchopleural fistula (BPF) is a problem that is difficult to manage and requires thoracotomy as a palliative measure, with daily treatment and recurring infections of the pleural cavity.
The existence of fistulas in the main bronchus means that it is impossible to close the thoracotomy cavity as it is chronically infected. Several techniques have been reported for closing fistulas1,2 (stents, coils, bioadhesives…) with uneven results.
The use of the Figulla® Flex device (Occlutech® Izasa, Werfen Group), which was originally designed for the closure of heart defects, has been described in this situation.3 Its double-umbrella design and central area with its smaller diameter make it ideal for becoming anchored in the fistula and sealing the existing tissue defects.
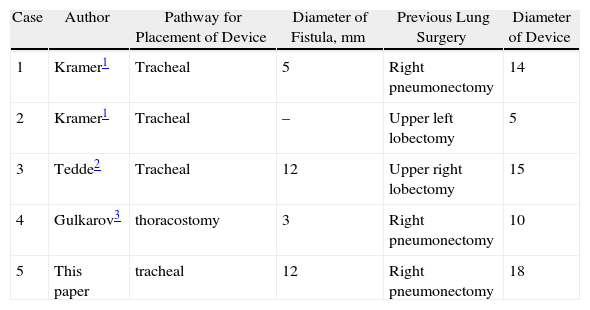
Very few cases have been described in the literature, and all of them recently (Table 1). We contribute a case of post-pneumonectomy right bronchial stump fistula that was closed using this method.
Cases Treated With Umbrella Devices for Closure of Post-surgical Bronchial Fistulas.
| Case | Author | Pathway for Placement of Device | Diameter of Fistula, mm | Previous Lung Surgery | Diameter of Device |
| 1 | Kramer1 | Tracheal | 5 | Right pneumonectomy | 14 |
| 2 | Kramer1 | Tracheal | – | Upper left lobectomy | 5 |
| 3 | Tedde2 | Tracheal | 12 | Upper right lobectomy | 15 |
| 4 | Gulkarov3 | thoracostomy | 3 | Right pneumonectomy | 10 |
| 5 | This paper | tracheal | 12 | Right pneumonectomy | 18 |
We present the case of a 67-year-old male who underwent right pneumonectomy some 19 months ago due to endobronchial squamous cell carcinoma (T2N0M0). Four weeks later, he was readmitted due to fever with productive cough. Diagnosed with bronchial stump fistula, thoracostomy was performed.
We confirmed the persistence of a stump fistula measuring 12mm in diameter with irregular edges that required closure with surgical compresses through the thoracostomy. The patient presented fair general health, with chronic respiratory failure and recurring infections. His baseline state and the oncological disease-free interval led us to consider closing the fistula with a Figulla® Flex device (Occlutech®).
Given the fact that it was impossible to correctly insert a double-lumen tracheal tube due to the great distortion of the tracheobronchial tree that was a consequence of the previous surgery and the retraction of the mediastinum, there was difficulty for ventilation with positive pressure due to the air leak through the BPF. Therefore, we carried out selective intubation of the left main bronchus, placing a tracheal tube through the left nasal cavity (preformed 6F), which was guided with a bronchoscope.
With a second bronchoscope inserted through the thoracostomy cavity, the fistula was located. This enabled us to insert a metallic guide through the bronchoscope inserted in the right nasal cavity to the bronchial fistula. Through the guide, the introducer sheath was inserted (12F diameter) with the 18-mm Figulla® Flex ASD (Occlutech® Ref 24ASD 18). Once it was within the fistula, the device was deployed (Fig. 1), but before it was released from the guide, X-ray confirmed that it was correctly placed. A nearly complete reduction of the bronchial air leak was observed. After extubation, the patient remained in the Intensive Care Unit for 24h and was sent home 48h after the procedure had been completed.

Please cite this article as: Galbis JM, et al. Cierre de fístula del bronquio principal tras neumonectomía con un dispositivo Figulla Flex Occlutech ASD. Arch Bronconeumol. 2012; 48: 137-8.







