


A 33-year-old man with no significant past medical history presented with a mediastinal mass that had been found incidentally on a chest CT examination performed as part of the investigation of a respiratory infection. Non-enhanced chest CT showed a prevascular mediastinal mass (Fig. 1A–C). Enhanced CT with coronal reconstruction (Fig. 1D–E) and 3D volumetric reconstruction (Fig. 1F) demonstrated a fusiform aneurysm of the brachiocephalic vein, extending to the superior vena cava, measuring 2.5cm×2.7cm×3.8cm; its neck was 1.1cm in diameter. A final diagnosis of left brachiocephalic vein aneurysm (BCVA) was made. Some treatment options were offered to the patient, especially antithrombotic treatments. The patient refused any kind of treatment, and is being followed on an outpatient basis. After 3 years, he remains asymptomatic.
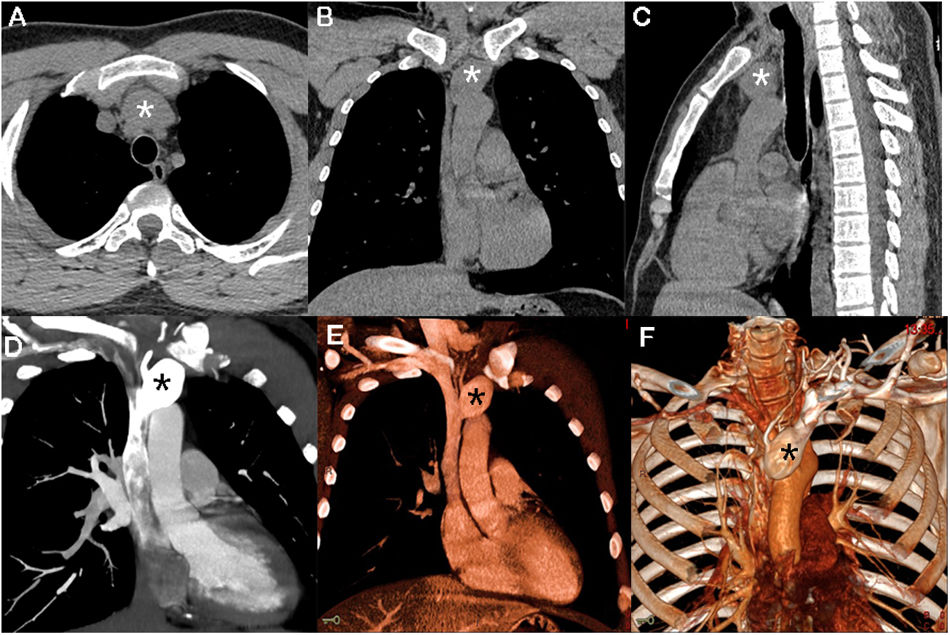
Non-enhanced chest CT (A–C) showed a prevascular mediastinal mass (asterisks). Enhanced CT with coronal reconstruction (D, E) and 3D volumetric reconstruction (F) demonstrated a fusiform aneurysm of the brachiocephalic vein, beginning 1.5cm distal to the internal jugular vein and extending to the superior vena cava (asterisks).
Aneurysms of the brachiocephalic (or innominate) vein are very rare. About 40 cases have been reported to date. They may be completely asymptomatic, presenting as incidental findings on imaging examinations or as a result of complications that they cause, including thromboembolism and venous obstruction, rupture, and compression of adjacent structures. The most common BCVA presentation is a widened mediastinum on a chest radiograph. The accurate diagnosis of a mediastinal aneurysm is essential to avoid complications secondary to biopsy or surgical intervention. Imaging is usually sufficient for the identification and characterization of such aneurysms.1,2
The two main types of BCVA are fusiform (comprising the majority of cases) and saccular. Treatment is largely determined by clinical presentation, morphological characteristics of the aneurysm (saccular or fusiform, condition of the neck and the size of the aneurysm), patient decisions, and surgical conditions. Current treatment approaches include conservative management and open surgery. Endovascular treatment is also becoming a therapeutic option. For larger saccular BCVA, even those that are asymptomatic, prophylactic surgical resection has been recommended. Fusiform aneurysms like that identified in our patient pose a much lower risk of complication and can be treated conservatively.1,2
Conflict of interestThe authors declare that they have no conflicts of interest to express.







