

Clinical severity of COVID-19 infections ranges widely, from asymptomatic or mild disease of the upper airways to pneumonia and acute respiratory distress syndrome (ARDS).1–3 We aim to describe biological features and outcomes of 240 patients admitted for SARS-CoV-2 pneumonia, as well as identify predictors of intensive care unit (ICU) admission (either direct admission or transfer to ICU within 96h of admission from emergency department), need for invasive mechanical ventilation (IMV) and in-hospital mortality.
For this retrospective, observational study, all consecutive patients with laboratory-confirmed SARS-CoV-2 infection and pneumonia (positive result by real-time polymerase chain reaction testing of a oropharyngeal plus nasopharyngeal sample4), who visited the emergency department and were subsequently admitted to the hospital between February 28th and April 21st, 2020, were included. Patients without pneumonia were excluded. The Institutional Ethics Board approved this study and due to its nature, waived the need for informed consent. Clinical outcomes were monitored until May 15th, 2020. Patients were divided into two groups: non-ICU and ICU-admitted (either direct admission or transfer to ICU within 96h of admission from emergency department).
Descriptive statistics were used for basic features of study data; appropriate statistical tests were performed to compare both groups. Univariate and multivariable binary logistic regression,5 multinomial logistic regression5 and Cox regression6 analyses were performed to identify variables associated with ICU admission, mechanical ventilation and in-hospital mortality, respectively.
Among the 800 patients admitted during the observation period for SARS-CoV-2, 465 (58%) patients had pneumonia. Of these patients, 225 were excluded from analysis due to outpatient care, inter-hospital transfer or unavailable data. The population therefore comprised 240 patients (115 non-ICU and 125 ICU-admitted [65% direct admission to ICU and 35% transfer to ICU within 96h of admission from emergency department]). The mean age was 57.7 ([standard deviation] [17.8]) years and 67% of all patients were male. The median (interquartile range [IQR]) duration of onset of symptoms to hospital admission was 7 (4; 8) days (Table 1 Panel A).
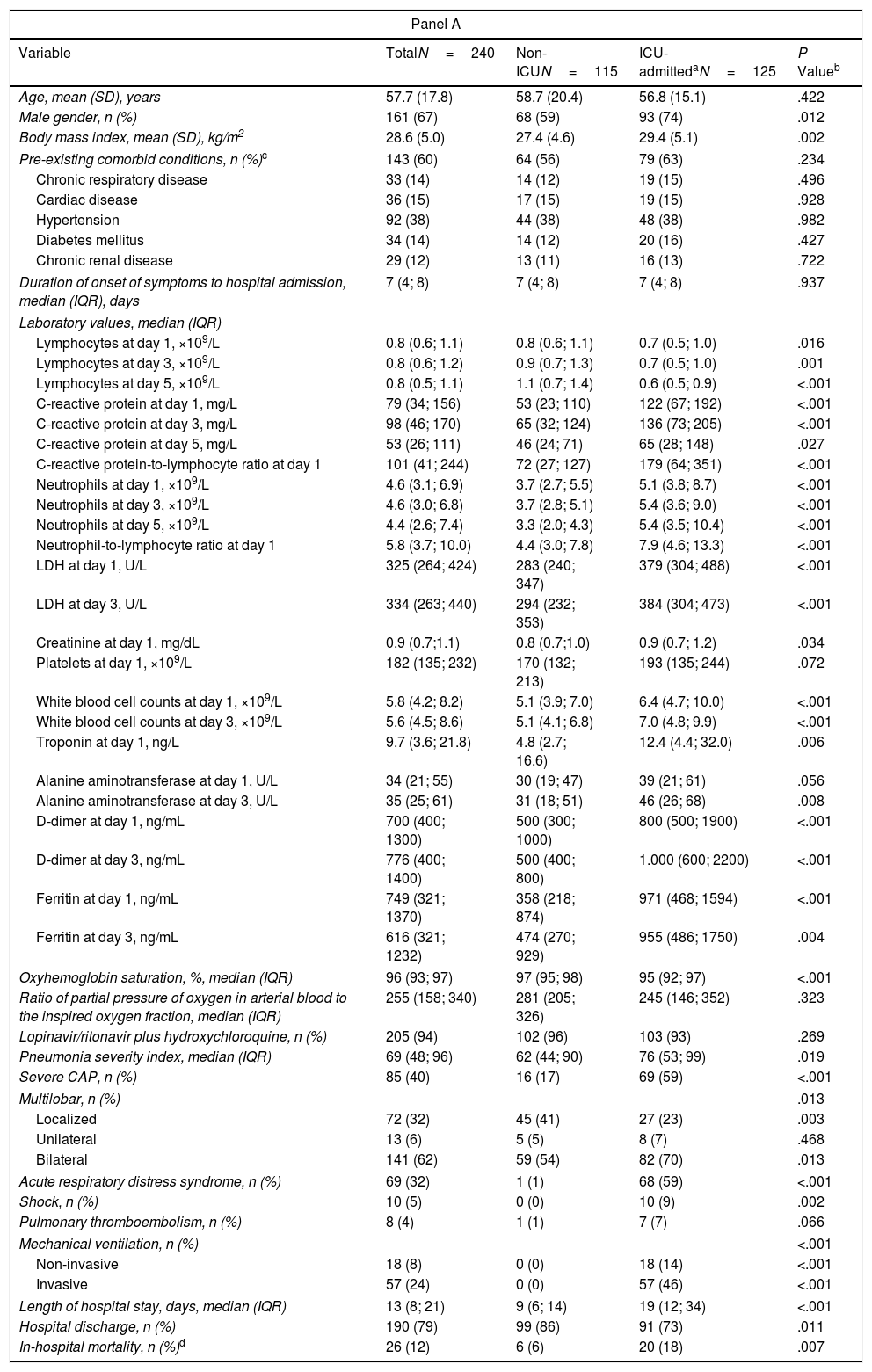
Clinical Features of Patients With COVID-19 Pneumonia Upon Admission (Panel A) and Significant Risk Factors for ICU Admission and Mechanical Ventilation Using Binary Logistic Regression and Multinomial Logistic Regression Analyses, Respectively (Panel B).
| Panel A | ||||
|---|---|---|---|---|
| Variable | TotalN=240 | Non-ICUN=115 | ICU-admittedaN=125 | P Valueb |
| Age, mean (SD), years | 57.7 (17.8) | 58.7 (20.4) | 56.8 (15.1) | .422 |
| Male gender, n (%) | 161 (67) | 68 (59) | 93 (74) | .012 |
| Body mass index, mean (SD), kg/m2 | 28.6 (5.0) | 27.4 (4.6) | 29.4 (5.1) | .002 |
| Pre-existing comorbid conditions, n (%)c | 143 (60) | 64 (56) | 79 (63) | .234 |
| Chronic respiratory disease | 33 (14) | 14 (12) | 19 (15) | .496 |
| Cardiac disease | 36 (15) | 17 (15) | 19 (15) | .928 |
| Hypertension | 92 (38) | 44 (38) | 48 (38) | .982 |
| Diabetes mellitus | 34 (14) | 14 (12) | 20 (16) | .427 |
| Chronic renal disease | 29 (12) | 13 (11) | 16 (13) | .722 |
| Duration of onset of symptoms to hospital admission, median (IQR), days | 7 (4; 8) | 7 (4; 8) | 7 (4; 8) | .937 |
| Laboratory values, median (IQR) | ||||
| Lymphocytes at day 1, ×109/L | 0.8 (0.6; 1.1) | 0.8 (0.6; 1.1) | 0.7 (0.5; 1.0) | .016 |
| Lymphocytes at day 3, ×109/L | 0.8 (0.6; 1.2) | 0.9 (0.7; 1.3) | 0.7 (0.5; 1.0) | .001 |
| Lymphocytes at day 5, ×109/L | 0.8 (0.5; 1.1) | 1.1 (0.7; 1.4) | 0.6 (0.5; 0.9) | <.001 |
| C-reactive protein at day 1, mg/L | 79 (34; 156) | 53 (23; 110) | 122 (67; 192) | <.001 |
| C-reactive protein at day 3, mg/L | 98 (46; 170) | 65 (32; 124) | 136 (73; 205) | <.001 |
| C-reactive protein at day 5, mg/L | 53 (26; 111) | 46 (24; 71) | 65 (28; 148) | .027 |
| C-reactive protein-to-lymphocyte ratio at day 1 | 101 (41; 244) | 72 (27; 127) | 179 (64; 351) | <.001 |
| Neutrophils at day 1, ×109/L | 4.6 (3.1; 6.9) | 3.7 (2.7; 5.5) | 5.1 (3.8; 8.7) | <.001 |
| Neutrophils at day 3, ×109/L | 4.6 (3.0; 6.8) | 3.7 (2.8; 5.1) | 5.4 (3.6; 9.0) | <.001 |
| Neutrophils at day 5, ×109/L | 4.4 (2.6; 7.4) | 3.3 (2.0; 4.3) | 5.4 (3.5; 10.4) | <.001 |
| Neutrophil-to-lymphocyte ratio at day 1 | 5.8 (3.7; 10.0) | 4.4 (3.0; 7.8) | 7.9 (4.6; 13.3) | <.001 |
| LDH at day 1, U/L | 325 (264; 424) | 283 (240; 347) | 379 (304; 488) | <.001 |
| LDH at day 3, U/L | 334 (263; 440) | 294 (232; 353) | 384 (304; 473) | <.001 |
| Creatinine at day 1, mg/dL | 0.9 (0.7;1.1) | 0.8 (0.7;1.0) | 0.9 (0.7; 1.2) | .034 |
| Platelets at day 1, ×109/L | 182 (135; 232) | 170 (132; 213) | 193 (135; 244) | .072 |
| White blood cell counts at day 1, ×109/L | 5.8 (4.2; 8.2) | 5.1 (3.9; 7.0) | 6.4 (4.7; 10.0) | <.001 |
| White blood cell counts at day 3, ×109/L | 5.6 (4.5; 8.6) | 5.1 (4.1; 6.8) | 7.0 (4.8; 9.9) | <.001 |
| Troponin at day 1, ng/L | 9.7 (3.6; 21.8) | 4.8 (2.7; 16.6) | 12.4 (4.4; 32.0) | .006 |
| Alanine aminotransferase at day 1, U/L | 34 (21; 55) | 30 (19; 47) | 39 (21; 61) | .056 |
| Alanine aminotransferase at day 3, U/L | 35 (25; 61) | 31 (18; 51) | 46 (26; 68) | .008 |
| D-dimer at day 1, ng/mL | 700 (400; 1300) | 500 (300; 1000) | 800 (500; 1900) | <.001 |
| D-dimer at day 3, ng/mL | 776 (400; 1400) | 500 (400; 800) | 1.000 (600; 2200) | <.001 |
| Ferritin at day 1, ng/mL | 749 (321; 1370) | 358 (218; 874) | 971 (468; 1594) | <.001 |
| Ferritin at day 3, ng/mL | 616 (321; 1232) | 474 (270; 929) | 955 (486; 1750) | .004 |
| Oxyhemoglobin saturation, %, median (IQR) | 96 (93; 97) | 97 (95; 98) | 95 (92; 97) | <.001 |
| Ratio of partial pressure of oxygen in arterial blood to the inspired oxygen fraction, median (IQR) | 255 (158; 340) | 281 (205; 326) | 245 (146; 352) | .323 |
| Lopinavir/ritonavir plus hydroxychloroquine, n (%) | 205 (94) | 102 (96) | 103 (93) | .269 |
| Pneumonia severity index, median (IQR) | 69 (48; 96) | 62 (44; 90) | 76 (53; 99) | .019 |
| Severe CAP, n (%) | 85 (40) | 16 (17) | 69 (59) | <.001 |
| Multilobar, n (%) | .013 | |||
| Localized | 72 (32) | 45 (41) | 27 (23) | .003 |
| Unilateral | 13 (6) | 5 (5) | 8 (7) | .468 |
| Bilateral | 141 (62) | 59 (54) | 82 (70) | .013 |
| Acute respiratory distress syndrome, n (%) | 69 (32) | 1 (1) | 68 (59) | <.001 |
| Shock, n (%) | 10 (5) | 0 (0) | 10 (9) | .002 |
| Pulmonary thromboembolism, n (%) | 8 (4) | 1 (1) | 7 (7) | .066 |
| Mechanical ventilation, n (%) | <.001 | |||
| Non-invasive | 18 (8) | 0 (0) | 18 (14) | <.001 |
| Invasive | 57 (24) | 0 (0) | 57 (46) | <.001 |
| Length of hospital stay, days, median (IQR) | 13 (8; 21) | 9 (6; 14) | 19 (12; 34) | <.001 |
| Hospital discharge, n (%) | 190 (79) | 99 (86) | 91 (73) | .011 |
| In-hospital mortality, n (%)d | 26 (12) | 6 (6) | 20 (18) | .007 |
| Panel B | |||
|---|---|---|---|
| ICU Admissiona,e,f,g | Multivariableh | ||
| Variable | OR | 95% CI | P Value |
| Body mass index:Overweight (≥25 and <30kg/m2) or obese (≥30kg/m2) | 2.61 | 1.31–5.20 | .006 |
| C-reactive protein-to-lymphocyte ratio at day 1 (+ 10 units)i | 1.05 | 1.02–1.07 | <.001 |
| Ferritin at day 1 (+100ng/mL)j | 1.05 | 1.02–1.08 | .002 |
| Mechanical Ventilationk,f,g | Non-invasive | Invasive | ||||
|---|---|---|---|---|---|---|
| Multivariablel | Multivariablel | |||||
| Variable | OR | 95% CI | P Value | OR | 95% CI | P Value |
| C-reactive protein-to-lymphocyte ratio at day 1 (+ 10 units)i | 1.02 | 0.99–1.05 | .219 | 1.04 | 1.02–1.06 | <.001 |
| Platelets at day 1 (+10×109/L)m | 1.09 | 1.03–1.15 | .001 | 1.02 | 0.98–1.06 | .338 |
| Ferritin at day 1 (+100ng/mL)j | 1.02 | 0.97–1.07 | .531 | 1.06 | 1.03–1.10 | <.001 |
Abbreviations: CAP, community-acquired pneumonia; CI indicates confidence interval; ICU, intensive care unit; IQR, interquartile range; LDH, lactate dehydrogenase; OR, odds ratio; SD, standard deviation.
Categorical variables were compared using the Chi-squared test or Fisher's exact test. Continuous variables were compared using the t-test or nonparametric Mann–Whitney test. The level of significance was set at 0.05 (two-tailed).
Calculated only for 213 patients who did not have a DNR, died prior to 15 May 2020 or were alive at discharge (102 in the non-ICU group and 111 in the ICU group), i.e. excluding patients who were still hospitalized or with a DNR. Five patients who died in less than 24h of admission were excluded.
Data is shown as estimated ORs (95% CIs) of the explanatory variables in the ICU group. The OR represents the odds that ICU admission will occur given exposure to the explanatory variable, compared to the odds of the outcome occurring in the absence of such exposure. P-values are based on the null hypothesis that all ORs relating to an explanatory variable equal unity (no effect).
We used the multiple imputation method for missing data in the univariate and multivariable analyses.
The variables analyzed in the univariate analysis were age, gender, body mass index, comorbidity, duration of onset of symptoms to hospital admission, C-reactive protein at day 1, lymphocytes at day 1, C-reactive protein-to-lymphocyte ratio at day 1, neutrophils at day 1, neutrophil-to-lymphocyte ratio at day 1, LDH at day 1, LDH-to-lymphocyte ratio at day 1, platelets at day 1, D-dimer at day 1, and ferritin at day 1. Factors showing an association in the univariate analyses (P<.25) were incorporated in the multivariable model. Final variable selection was performed using the backward stepwise selection method (likelihood ratio) (Pin<0.05, Pout>0.10). Single collinearity was evaluated using the Pearson correlation (r); multicollinearity was examined by means of the variance inflation factor (VIF).
Hosmer–Lemeshow goodness-of-fit test for the multivariable model, P=.603. Area under the ROC curve for the multivariable model, AUC=0.77 (95% CI 0.71–0.83). Linear relationships between continuous predictors and logit (log odds) were confirmed by the Box-Tidwell test. Internal validation of the multivariable model using ordinary nonparametric bootstrapping with 1000 samples demonstrated robust results for the three variables included in the model, with small 95% CIs around the original coefficients.
Data is shown as estimated ORs (95% CIs) of the explanatory variables in non-invasive mechanical ventilation and invasive mechanical ventilation groups. The OR represents the odds that the need for non-invasive mechanical ventilation or invasive mechanical ventilation will occur given exposure to the explanatory variable, compared to the odds of the outcome occurring in the absence of such exposure. P-values are based on the null hypothesis that all ORs relating to an explanatory variable equal unity (no effect).
Model characteristics: likelihood ratio Chi-squared test, P=.637; R2 coefficients=0.24 (Cox and Snell), 0.30 (Nagelkerke). AUC=0.73 (95% CI 0.61–0.85) for non-invasive mechanical ventilation group and AUC=0.80 (95% CI 0.74–0.87) for invasive mechanical ventilation group. Linear relationships between continuous predictors and logit (log odds) were confirmed with the Box-Tidwell test. Internal validation of the multivariable model using ordinary nonparametric bootstrapping with 1000 samples demonstrated robust results for the three variables included in the model, with small 95% CIs around the original coefficients.
When compared to non-ICU patients, ICU-admitted patients were more likely to be men and have higher body mass index (BMI). ICU-admitted patients also showed higher levels of creatinine, C-reactive protein, neutrophils, lactate dehydrogenase (LDH), white blood cell count, troponin, D-dimer, ferritin, and troponin. Similarly, we observed elevated C-reactive protein-to-lymphocyte, neutrophil-to-lymphocyte ratio and lower lymphocyte count and oxygen saturation upon admission (first 24h) in ICU-admitted patients. During hospitalization (days 3–5), those admitted to the ICU developed severe lymphopenia more frequently (0.6 vs. 1.1; P<.001) than non-ICU patients. Levels of C-reactive protein, neutrophils, white blood cell count, alanine aminotransferase (ALT) and LDH, D-dimer and ferritin were higher in ICU-admitted patients over time (day 3–5) (Table 1-Panel A).
No significant differences were observed in therapies administered to ICU-admitted and non-ICU patients. Most patients received lopinavir/ritonavir plus hydroxychloroquine plus azithromycin upon hospital admission (92% vs. 94%, P=.558).
BMI, ferritin levels and the C-reactive protein-to-lymphocyte ratio upon admission were independently associated with ICU admission (either, direct ICU admission and transfer to ICU in the first 96h of admission) in the multivariable analysis (Table 1-Panel B). For patients who were direct to ICU admission, BMI (overweight or obese: odds ratio [OR] 2.13 [95% confidence interval [CI] 0.94–4.85]), ferritin levels (+100ng/ml: OR 1.06 [95% CI 1.02–1.09]), the C-reactive protein-to-lymphocyte ratio (+10 units: OR 1.05 [95% CI 1.03–1.07]) and platelets levels (+10×109/L: OR 1.05 [95% CI 1.00–1.09]) were independently associated with ICU admission (AUC=0.78 [95% CI 0.72–0.84]), whereas for patients transferred to ICU within 96h of admission from emergency department, BMI (overweight or obese: OR 3.33 [95% CI 1.28–8.67]), ferritin levels (+100ng/ml: OR 1.04 [95% CI 1.00–1.08]), the C-reactive protein-to-lymphocyte ratio (+10 units: OR 1.04 [95% CI 1.01–1.06]) and platelets levels (+10×109/L: OR 0.94 [95% CI 0.88–0.99]) were independently associated with ICU transfer(AUC=0.70 [95% CI 0.62–0.78]).
Furthermore, ferritin levels and the C-reactive protein-to-lymphocyte ratio upon admission were independently associated with the need for IMV (Table 1-Panel B).
After excluding patients who were still hospitalized and those with do-not-resuscitate orders, in-hospital mortality was 12%, with differences observed between groups (18% in the ICU-admitted group vs. 6% in the non-ICU group, P=.007). Results from the multivariable analysis showed that age (hazard ratio [HR], 1.05; 95% CI, 1.02–1.08), platelets (HR, 0.96; 95% CI, 0.92–1.01), ferritin (HR, 1.05; 95% CI, 1.00–1.05), and D-dimer levels (HR, 1.01; 95% CI, 1.01–1.03), were independently associated with the risk of in-hospital mortality (AUC=0.73 [95% CI 0.62–0.83]).
This cohort study provides the first description of COVID-19 pneumonia in Barcelona, Spain. Patients with higher BMI and elevated levels of C-reactive protein-to-lymphocyte ratio and ferritin upon admission presented with an increased risk of ICU admission. This may reflect both a stronger systemic inflammatory response and the existence of immunological dysregulation in severe COVID-19.8 Similarly, it is well known that obesity is a risk factor for severe infection, related to low-grade chronic inflammation and has a potential effect on immune responses.9
Interestingly, we observed that platelet levels were an additional variable independently associated with ICU admission in both patients who went directly to the ICU and those who transferred to the ICU within 96h of admission to the emergency department. These results support the fact that a decrease in platelet count usually indicates multiple organ dysfunction, and provides prognostic information.10
Twenty-four percent of our patients underwent IMV. Notably, we found that C-reactive protein-to-lymphocyte ratio and ferritin levels upon admission were independently associated with the need for IMV. Previous studies reported that higher ferritin levels were associated with a clinical deterioration in patients with COVID-19. A meta-analysis also reported that both the neutrophil-to-lymphocyte ratio and C-reactive protein-to-lymphocyte ratio significantly increased in severe COVID-19 cases.7 However, this cohort study is the first of its nature to explore the value of the C-reactive protein-to-lymphocyte ratio in patients with COVID-19 pneumonia. The level of C-reactive protein-to-lymphocyte ratio reflects the balance between the systemic inflammatory and immune responses. An elevated C-reactive protein-to-lymphocyte ratio indicates an increase in the systemic inflammatory response and a decrease in the immune response. As we observed in our study, elevated C-reactive protein-to-lymphocyte ratio is an important predictor factor for both ICU admission (both direct admission and transfer to ICU) and need for IMV.
The results of our study have important clinical implications and strengths. As C-reactive protein-to-lymphocyte ratio could be quickly calculated based on a routine blood test performed upon admission, clinicians may be able to identify high-risk patients with COVID-19 during the early stages of the infection. The main limitation of the study is that it includes patients from a single center. Notwithstanding, important preliminary results concerning risk factors for ICU admission and need for IMV in patients with COVID-19 pneumonia are provided.
Early recognition of easily obtainable markers upon hospital admission such as serum ferritin, D-dimer, platelet count and the C-reactive protein-to-lymphocyte ratio could help identify and prioritize patients with a higher probability for ICU admission (both direct admission and transfer to ICU) and need of IMV during the course of hospitalization.
FundingThis study was supported by CIBER de Enfermedades Respiratorias (CIBERES CB06/06/0028), and by 2009 Support to Research Groups of Catalonia 911, IDIBAPS.
Conflict of InterestThe authors declare that they have no conflicts of interest.
We are indebted to the nursing staff and the attending physicians of our hospital for their cooperation in this study. Dr Cillóniz is the recipient of a postdoctoral grant (Strategic plan for research and innovation in health; ERIS 2016–2020), the SEPAR fellowship 2018, and a grant from the Fondo de Investigación Sanitaria (PI19/00207).
Josep Mensa, Pedro Castro, José Antonio Martínez, Felipe García, Laura Morata, Oriol Sibila, Natalia Rodríguez, Mariana Chumbita, Nicol Garcia-Pouton, Juan Ambrosioni, Marta Hernández, Daiana Agüero, Berta Torres, Sara Fernández, Laura Linares, Fernanda Meira, Irene Macaya, David Nicolas, Laia Albiach, Pedro Puerta, Alex Almuedo, José Muñoz, Monserrat Sola and Celia Cardozo (Hospital Clinic-IDIBAPS, University of Barcelona, Barcelona, Spain)
Dr. Cilloniz, Dr. Torres, Dr. Amaro, Dr. Soler are members of the Spanish Society of Pneumology and Thoracic Surgery (SEPAR) listed in Appendix A.







