

Intra-thoracic parathyroid glands is an unusual presentation (6–16%) of primary hyperparathyroidism,1 with most patients being asymptomatic during diagnosis.2
Surgical resection is indicated for symptomatic ectopic parathyroid adenomas or if calcium levels exceed 10mg/dl in the asymptomatic patients.
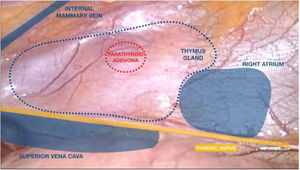
Moreover, intra-thoracic adenomas need careful surgical planning to achieve complete surgical excision. If any tissue is left, hyperparathyroidism persists. Pre-operative Sestamibi scintigraphy evaluates if patient has single or multi-gland disease.2 Scintigraphy localization can be done pre & intraoperative as shown in the video.
Thymectomy is done by blunt and en-bloc dissection using ultrasonic scalpel avoiding capsular rupture that can lead in potential seeding of cells increasing the incidence of local recurrence.
The removal of ectopic mediastinal parathyroid adenoma using VATS has been described in case reports and shows fewer complications than other procedures, with the post-operative benefits of minimally invasive surgery. One of the causes of surgical failure is the inadequate resection of the adenoma, which can be avoided with the use of radioguided surgery.
Finally, the most common complications in the resection of mediastinal adenomas are the lesion of the recurrent laryngeal nerve and hypoparathyroidism that can be prevented measuring pre and post-operative PTH levels.
FundingNo funders pertaining to this article.







