



This study aims to analyze trends in venous thromboembolism (VTE) mortality in the Spanish Autonomous Communities (ACs) from 1999 to 2022, with a focus on identifying regional disparities and informing targeted public health interventions.
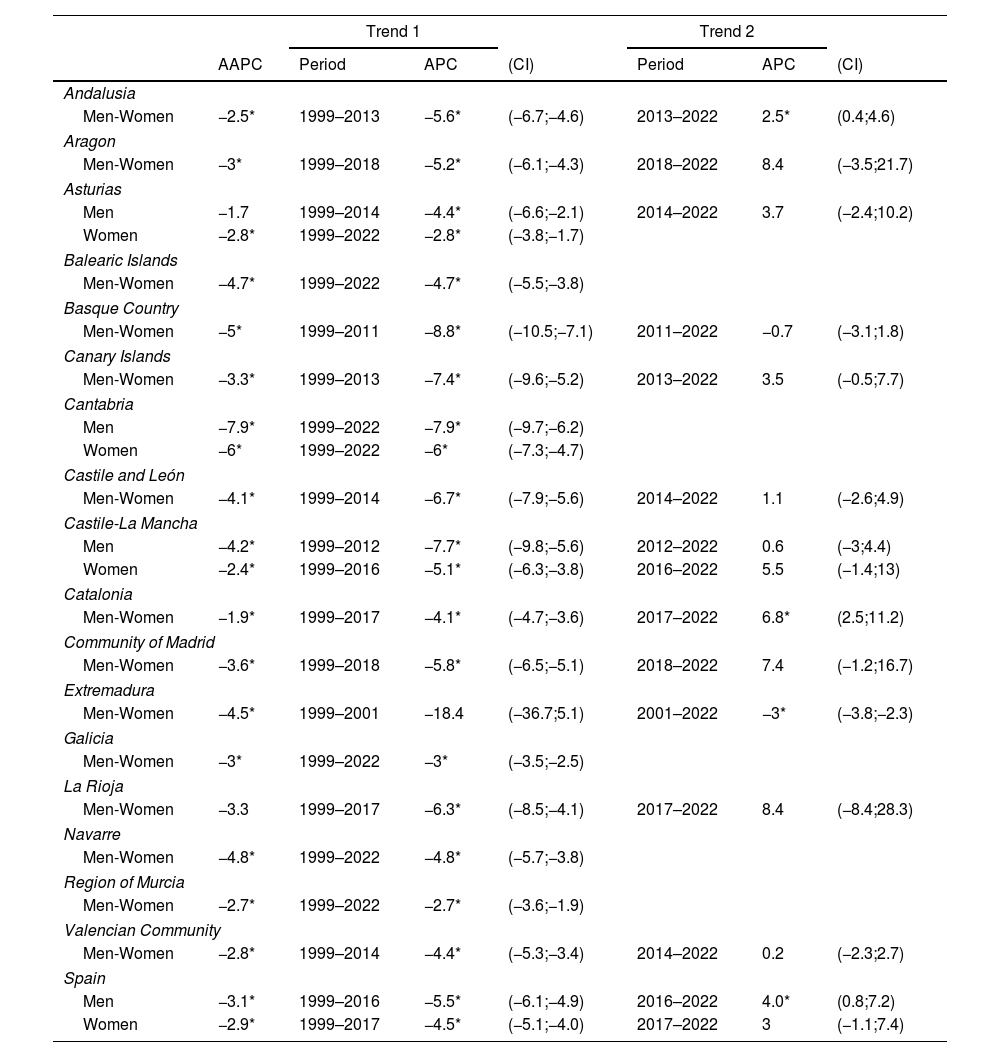
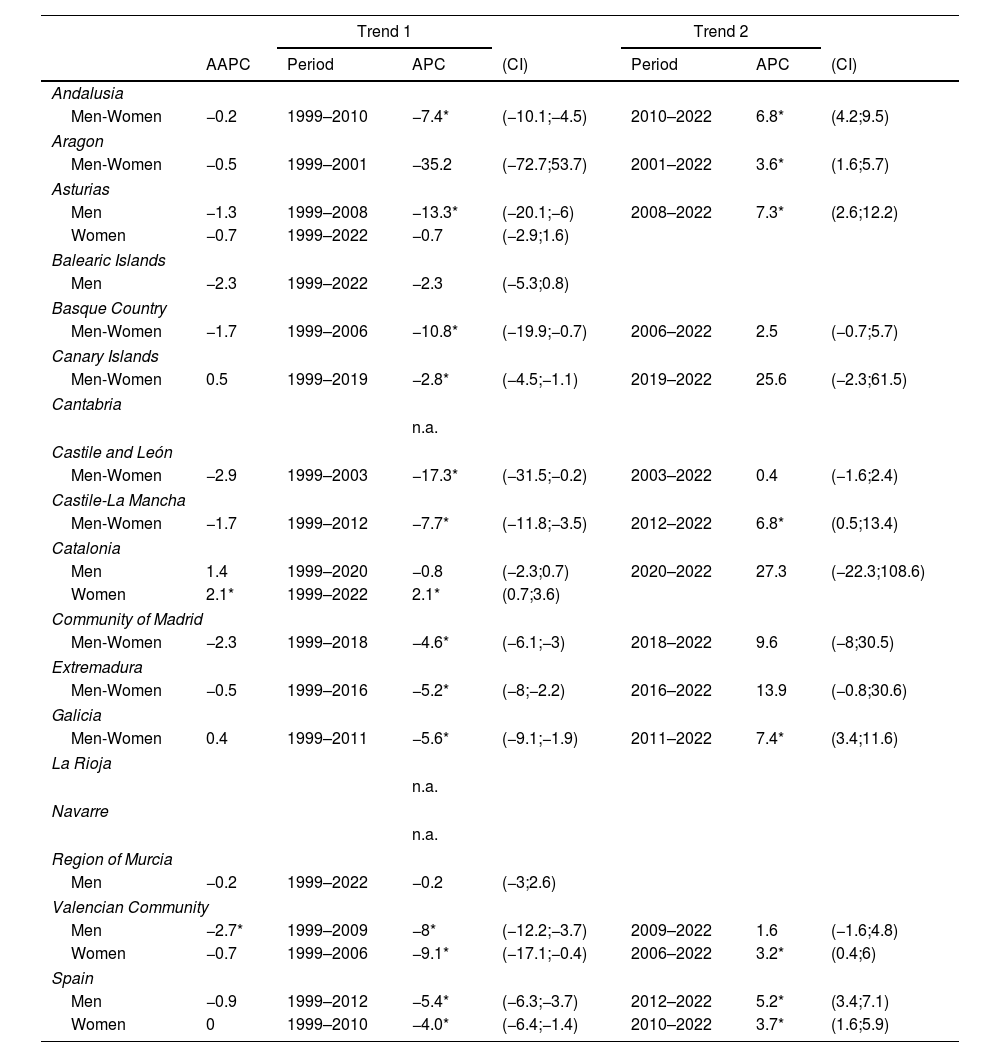
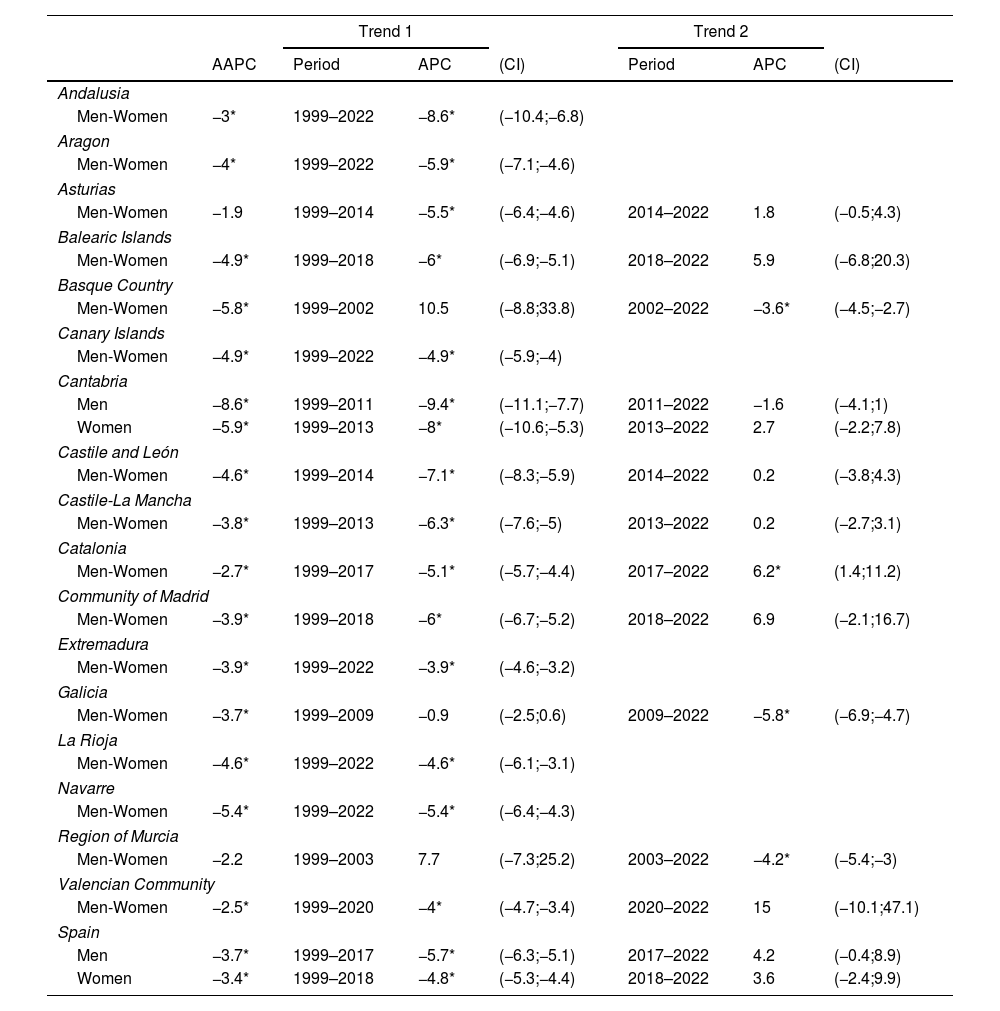
MethodsAge-standardized mortality rates (ASMRs) were calculated using the European standard population as a reference. Joinpoint regression analysis was employed to identify significant changes in mortality trends, and geographical analysis was conducted using Bayesian inference to assess regional variations in mortality risk.
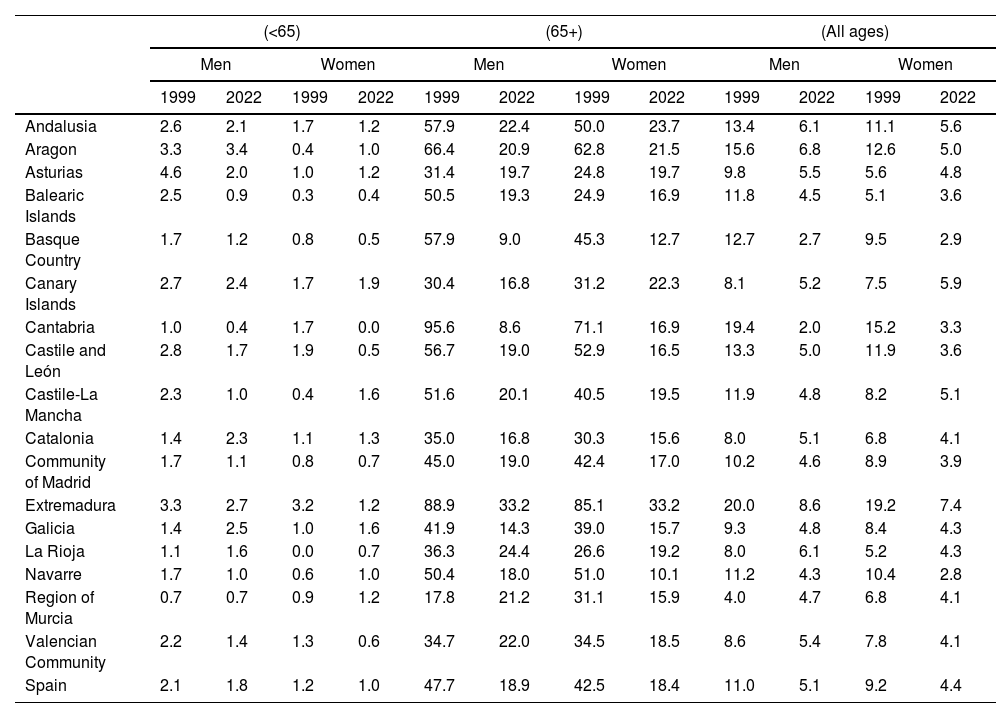
ResultsFrom 1999 to 2022, Spain recorded 59,515 VTE-related deaths, with a higher proportion in women (59.4%) compared to men (40.6%). On a nationwide scale, VTE ASMRs showed a general decline for both men and women, with rates decreasing from 11.0 to 5.1 per 100,000 in men and from 9.2 to 4.4 per 100,000 in women. However, this decline was not uniform across all regions or demographic groups. Notably, mortality rates among younger individuals, particularly men, increased during the study period, highlighting the need for targeted interventions. Analysis revealed significant regional disparities, with higher mortality risks observed in Extremadura, Aragon, Navarre, and Andalusia, particularly for women.
ConclusionsThis study provides valuable insights into the complex landscape of VTE mortality in Spain. While the overall decline in mortality is encouraging, persistent regional disparities and rising rates among younger individuals underscore the need for ongoing surveillance and targeted interventions.








