


A pulmonary sequestration is a lung tissue mass that is not connected with the central respiratory tract that receives its arterial blood supply from the systemic circulation.
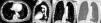
We present the case of a 76-year-old woman, reporting with no personal history of interest, with an incidental finding of a left retrocardiac mass during a routine pre-operative workup. The study was extended to include computed tomography (CT) with intravenous contrast, which revealed a well-outlined soft tissue mass in the postero-inferior region of the left hemithorax (Fig. 1A) that was supplied with arterial blood from the descending thoracic aorta (Fig. 1B) and drained into the left hemiazygos vein (Fig. 1C and D).
Pulmonary sequestrations are divided into two types: intralobar and extralobar. Intralobular sequestrations are acquired lesions, possibly resulting from chronic bronchial obstruction or pneumonia. 98% occur in the lower lobes and they are characterized by not having their own pleura.1 The arterial irrigation comes from an artery of the systemic circulation system, while the venous drainage is through the pulmonary circulation. The highest incidence of intralobular sequestration is found in young adults, and symptoms usually include repeated infections.
Extralobar sequestrations are congenital lesions that are mostly detected in children, although they may also be detected during the prenatal period using ultrasound.2,3 60% are located in the left hemithorax and they are characterized by having their own pleura. Arterial blood is supplied by the systemic circulation, while the venous return is what differs from intralobular sequestration as it is done through the general circulation. Extralobar sequestrations are usually asymptomatic, although they are frequently associated with other congenital anomalies such as diaphragmatic hernia or congenital heart disease.4
Sequestration is typically seen on chest radiographs as focal opacities that are either well or poorly defined. Extralobar sequestration tends to be adjacent to the mediastinum and therefore can be confused with mediastinal tumors. Intralobular sequestration may contain air, present poorly-defined edges and imitate pneumonia or pulmonary abscess. On CT, emphysema is frequently observed adjacent to this type of sequestration.
The key to its diagnosis is the visualization of the blood supply through the general arterial circulation, which differentiates sequestration from bronchogenic cysts, lobar atelectasis, necrotizing pneumonia or other parenchymal anomalies.5
Please cite this article as: Mayoral-Campos V, et al. Secuestro pulmonar. Arch Bronconeumol. 2013;49:129-30.







