




A 3-year-old pediatric patient was referred to our hospital with a history of recurrent respiratory infections and dry nocturnal cough following respiratory bronchiolitis at 5 months. On physical examination, she had mild tachypnea, subcostal and sternal retractions, and some bilateral crackling rales. A chest X-ray showed hyperinflation of both hemithoraxes and increased perihilar density (Fig. 1). Chest computed tomography (CT) scan was performed, showing areas of ground glass density in both lungs, more marked in the lingula and middle lobe (Figs. 1 and 2). An acute respiratory process was assumed, and symptomatic treatment with follow-up was prescribed. In the following months, several studies (autoimmunity, cystic fibrosis, pulmonary scintigraphy) were performed and found to be normal, and several drugs (mucolytics, β2 agonists, corticosteroids, and antibiotic therapy) were administered, but only partial symptomatic relief was achieved. A year later, a new CT was performed that showed persistence of lung findings, at which time the patient was diagnosed with neuroendocrine hyperplasia of infancy (NEHI).
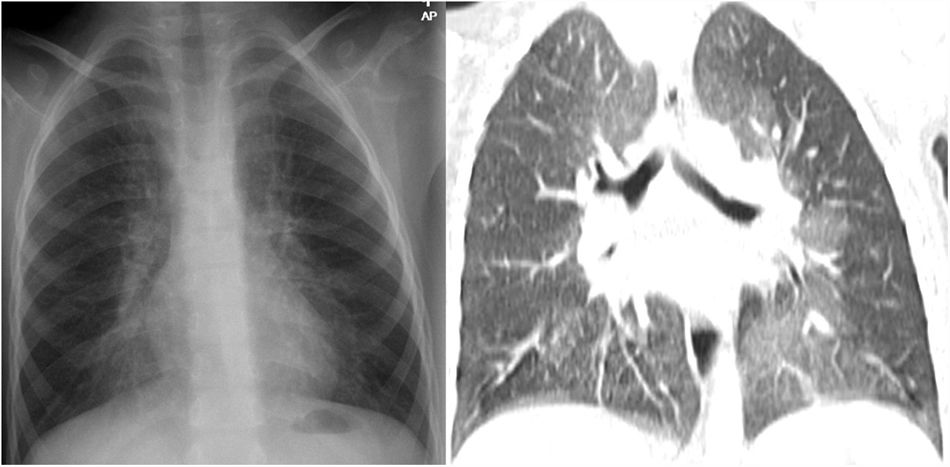
Plain X-ray of the chest (A). Hyperinflation of both hemithoraxes and increased lung parenchyma density in the perihilar region. Chest CT, coronal reconstruction (B). Areas with a ground glass pattern affecting predominantly the middle lobe and the lingula, showing the typical distribution pattern of neuroendocrine hyperplasia of infancy.
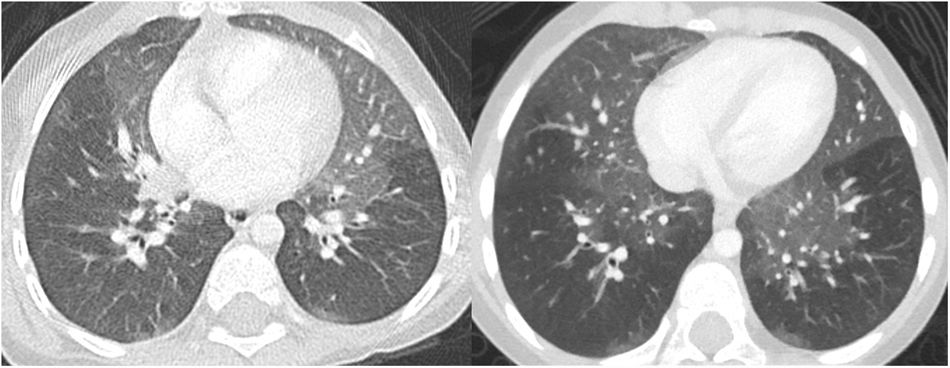
NEHI is a type of interstitial lung disease that usually occurs before the age of 2, presenting with tachypnea, crackles, chest retractions, and hypoxemia1,2. The appearance on CT is characterized by a mosaic attenuation pattern with patchy areas and ground glass density affecting 4 or more lobes, typically the lingula and middle lobe. In certain cases, consistent clinical signs and functional tests may permit diagnosis of NEHI without the need for a lung biopsy1,2. The recommended treatment is supportive, with oxygen therapy and prevention measures2.
Please cite this article as: Láinez Ramos-Bossini AJ, Ruiz de Arévalo Á, Ferrer Soriano JF. Hiperplasia neuroendocrina de la infancia: diagnóstico por imagen. Arch Bronconeumol. 2021;57:587.







