

Transsexuality is characterized by the discordance between gender identity and biological sex.1 The transsexualization process can take up to 10 years, causing suffering to the transsexual person as they begin to coexist for a long time with their chest dysphoria.2
To minimize or change the appearance of breasts, transgender men can compress their breasts with a chest binder.3,4 Despite any symptoms, transgender men continue the device use as a gender expression or identity,4,5 but the mastectomy could be a better choice to ensure health, safety and quality of life in these subjects.
The continuous use of binder can cause lesions or discomfort,4 but the related physical damage is still not quantified. With the hypothesis that the use of the binder may impair lung function due to the containment force and restriction on the expansion of the chest and lungs, this study aimed to compare the effect of using the binder on lung function, speech, and voice production in transsexual men.
This is an observational, cross-sectional, randomized, and blind pilot study approved by the Human Research Ethics Committee of the Institution (CAAE n° 30747120.0.0000.5440), which assessed a group of 15 transgender men who were in clinical follow-up at the Communication and Voice Outpatient Clinic for Transgenders and Transvestites, with an average age of 25±4 years and BMI of 27.13±6.16kg/m2, and were included according to the following inclusion criteria: over 18 years old, who had not undergone mastectomy surgery and used the binder daily.
Subjects were evaluated by spirometry and impulse oscillometry system (IOS) and then were submitted to the analysis of the aspects of communication and respiratory coordination, with and without the binder, wearing a dark cape around the chest to blind the evaluator about volunteer condition. The statistical analysis was also performed by a blind evaluator.
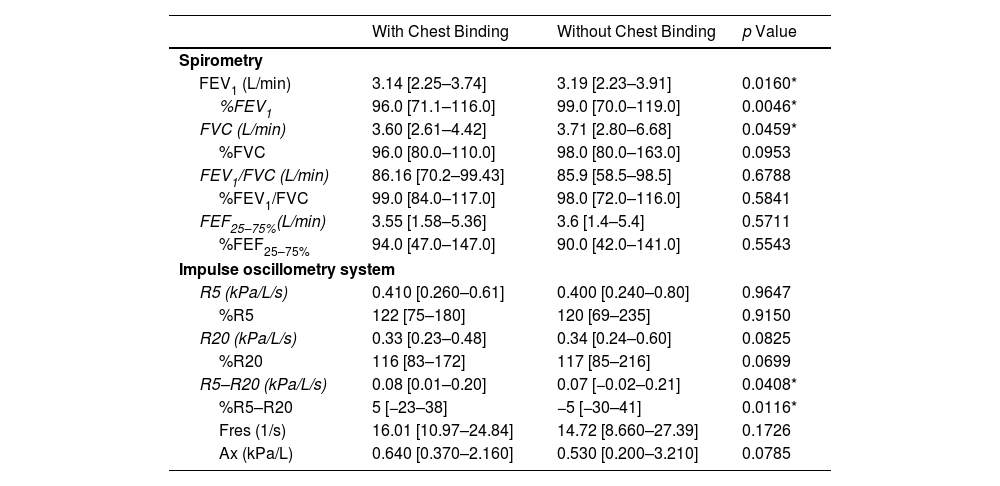
Our spirometry results showed that all participants had normal lung function with and without the binder; however, statistically significant lower FEV1, %FEV1, and FVC (p<.05) wearing binder. For IOS results, it was shown that the R5–R20 and %R5–R20 values were higher using binder, indicating an increase in peripheral airway resistance (Table 1).
Spirometric and Impulse Oscillometry System Data (n=15).
| With Chest Binding | Without Chest Binding | p Value | |
|---|---|---|---|
| Spirometry | |||
| FEV1 (L/min) | 3.14 [2.25–3.74] | 3.19 [2.23–3.91] | 0.0160* |
| %FEV1 | 96.0 [71.1–116.0] | 99.0 [70.0–119.0] | 0.0046* |
| FVC (L/min) | 3.60 [2.61–4.42] | 3.71 [2.80–6.68] | 0.0459* |
| %FVC | 96.0 [80.0–110.0] | 98.0 [80.0–163.0] | 0.0953 |
| FEV1/FVC (L/min) | 86.16 [70.2–99.43] | 85.9 [58.5–98.5] | 0.6788 |
| %FEV1/FVC | 99.0 [84.0–117.0] | 98.0 [72.0–116.0] | 0.5841 |
| FEF25–75%(L/min) | 3.55 [1.58–5.36] | 3.6 [1.4–5.4] | 0.5711 |
| %FEF25–75% | 94.0 [47.0–147.0] | 90.0 [42.0–141.0] | 0.5543 |
| Impulse oscillometry system | |||
| R5 (kPa/L/s) | 0.410 [0.260–0.61] | 0.400 [0.240–0.80] | 0.9647 |
| %R5 | 122 [75–180] | 120 [69–235] | 0.9150 |
| R20 (kPa/L/s) | 0.33 [0.23–0.48] | 0.34 [0.24–0.60] | 0.0825 |
| %R20 | 116 [83–172] | 117 [85–216] | 0.0699 |
| R5–R20 (kPa/L/s) | 0.08 [0.01–0.20] | 0.07 [−0.02–0.21] | 0.0408* |
| %R5–R20 | 5 [−23–38] | −5 [−30–41] | 0.0116* |
| Fres (1/s) | 16.01 [10.97–24.84] | 14.72 [8.660–27.39] | 0.1726 |
| Ax (kPa/L) | 0.640 [0.370–2.160] | 0.530 [0.200–3.210] | 0.0785 |
Data were expressed by median, minimum and maximum. FEV1: forced expiratory volume in the first second, FVC: forced vital capacity, FEV1/FVC: Tiffeneau index, FEF25–75%: mean forced expiratory flow. R5: resistance at 5Hz, R20: resistance at 20Hz, R5–R20: peripheral airway resistance, Fres: resonant frequency, Ax: reactance area.
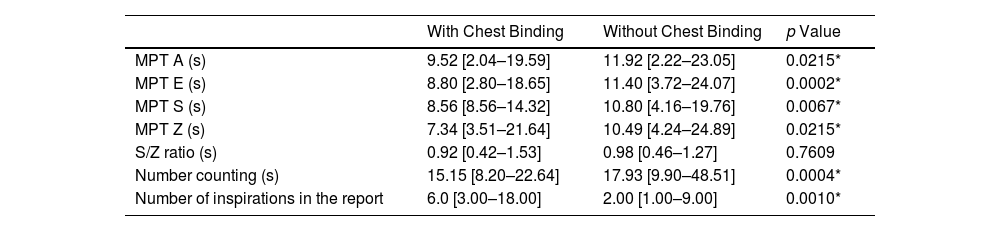
Regarding communication assessments, statistically significant differences were obtained for all variables of maximum phonation time – MPT (vowels and consonants), number count, and number of inspirations in the report (p<.05) (Table 2). We obtained a reduction in the MPT of vowels (A and E) and consonants (S and Z), counting numbers and the number of inspirations per report. There were no vocal changes in acoustic measurements, and all participants maintained a male voice frequency pattern between 80 and 150Hz.6
Maximum Phonation Time (Vowels and Consonants), Number Count, and Number of Inspirations in the Report Data (n=15).
| With Chest Binding | Without Chest Binding | p Value | |
|---|---|---|---|
| MPT A (s) | 9.52 [2.04–19.59] | 11.92 [2.22–23.05] | 0.0215* |
| MPT E (s) | 8.80 [2.80–18.65] | 11.40 [3.72–24.07] | 0.0002* |
| MPT S (s) | 8.56 [8.56–14.32] | 10.80 [4.16–19.76] | 0.0067* |
| MPT Z (s) | 7.34 [3.51–21.64] | 10.49 [4.24–24.89] | 0.0215* |
| S/Z ratio (s) | 0.92 [0.42–1.53] | 0.98 [0.46–1.27] | 0.7609 |
| Number counting (s) | 15.15 [8.20–22.64] | 17.93 [9.90–48.51] | 0.0004* |
| Number of inspirations in the report | 6.0 [3.00–18.00] | 2.00 [1.00–9.00] | 0.0010* |
Data were expressed by median, minimum, and maximum. MFT: maximum phonation time; MPT A: maximum phonation time of the vowel /a/; MPT E: maximum phonation time of the vowel /e/; MPT S: maximum phonation time of the consonant /s/; MPT Z: maximum phonation time of the consonant /z/; S/Z ratio: relationship established between the maximum production of the fricative phonemes /s/ and /z/.
To the best of our knowledge, there are no studies that have investigated the effects of the use of binder on the communication and respiratory function, and voice production of transgender men, as proposed in our protocol. Currently, the method of compressing breast tissue with different types of binders is widely used by transgender men to deal with gender dysphoria.4 It is known that such “bandages” can compromise health, triggering chest and abdominal pain, weakness and fatigue, musculoskeletal and neurological disorders, in addition to respiratory conditions (cough, respiratory infections, and shortness of breath), or skin lesions, already described by Peitzmeier et al. (2017).4
The chronic use of this “external” compression of the chest could influence lung function and could, therefore, lead to pulmonary restriction and respiratory complications.7 Our results showed, using refined research methodology with a blind evaluator, that there is a negative impact on lung volume and respiratory system resistance, which also compromises, in a more significant way, their communication.
Spirometry is the gold standard test to evaluate lung function, capable of identifying restrictive or obstructive patterns by measuring lung volumes and flows.8 To date, only one study, published in abstract form, has investigated the occurrence of respiratory deficits caused by the use of binder in transgender individuals through spirometry tests performed with and without the use of the device and the authors observed a statistically significant decrease in FVC values in the examination performed with binder.9 In our study, the spirometry tests of all volunteers were within normal limits; however, it was possible to observe that in tests with the binder, the FEV1 and FVC values were significantly reduced, confirming the results of Cumming and collaborators.9 It is worth noticing that the differences obtained in our study are not clinically relevant, but they suggest that, depending on the compression force, time of use, level of physical activity, and ventilatory demand, these changes may have harmful effects.
In addition, the IOS allows a compartmentalized analysis of the respiratory system in early stages and can contribute to understanding changes caused by binder compression.10–12 This tool evaluates the mechanical properties of the airways and lung parenchyma by effort-independent maneuvers.13–15 Our results demonstrated that R5–R20 and %R5–R20 measurements increased significantly in assessments using the binder, suggesting that this breast containment mechanism negatively influences peripheral airway resistance. To our knowledge, this is the first study that evaluated the resistance of the respiratory system in transgender men who use binder, confirming the negative effect of the device and the imposition of an overload on the respiratory system.
The MPT is a measurement used to evaluate the ability to control the aerodynamic forces of the respiratory system and the myoelectric forces of the larynx by sustaining the emission of a sound or chained speech in a single exhalation.6 In our sample, we had a normal standard of MPT for the participants with and without the use of binder; however, there was a significant decrease in the measurements of the maximum time of the vowels /A/ and /E/, and of the consonants /S/ and /Z/ when participants were using the device.
There was no significant difference when we compared the S/Z ratio with and without the binder, which shows that the glottic closure competence was not changed with the presence or absence of the device. The S/Z ratio is established between the maximum production of the fricative phonemes /s/ and /z/, which allows identifying the occurrence of muscular hypercontraction component or lack of coaptation of the vocal folds in subjects with functional and organic-functional dysphonia.6,16,17
During the spontaneous speech and chaining in speech tasks, collected by counting inspirations during speech and counting numbers, it was possible to identify a significant decrease in measures of time and quantity with the binder. Currently, there are no regulations for spontaneous speech and connected speech tasks, as each person has their individualism in speech. However, we could identify a significant decrease associated with the use of chest binders, which highlights the importance of standardized and comparative assessments.
The sample size should be noted as a limitation of the study and requires a careful interpretation of the results. Also, no multivariate analysis was performed during exercise or other activities that increase the ventilatory demand.
Thus, we conclude that chest binding affects lung function and increases airway resistance, in addition to causing speech impairments, such as decreasing maximum phonation time and increasing inspiration in spontaneous speech and the voice of transgender subjects. These changes, at rest, can cause greater limitations with increased ventilatory demand, as during any physical activity, which is consistent with the complaints reported by users, and, therefore, accessibility to surgery can reduce the damage to the physical and mental health of transsexual men binder users. However, further studies are needed to confirm these findings.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors’ ContributionsPerossi, J: literature research, study design, data collection, analysis of data, manuscript preparation and review of manuscript.
Prudêncio, JLG: literature research, study design, data collection, manuscript preparation.
Wolf, AE: literature research, study design, analysis of data, manuscript preparation, review of manuscript.
Belarmino, HS: literature research, data collection, manuscript preparation.
Santos, DO: literature research, data collection, analysis of data.
Gastaldi, AC: literature research, study design, analysis of data, manuscript preparation, review of manuscript.
Conflicts of InterestThe authors declare no conflicts of interest.
Artificial Intelligence InvolvementThe authors declare that they haven’t used Artificial Intelligence (AI)-assisted technologies (such as Large Language Models [LLMs], chatbots, or image creators) in the production of submitted work.
The authors want to thank the Ribeirao Preto Medical School Clinical Hospital, the Respiratory Evaluation Laboratory, and the University of Sao Paulo for the local and equipment support for this study and the participants who agreed to volunteer.







