

To describe the clinical characteristics and risk factors of patients with chest trauma, and to evaluate their correlation with the development of complications.
MethodsDescriptive, prospective and analytical study of a patient cohort with chest trauma who underwent follow-up for a period of 30days. Excluded from the study were those patients with moderate to severe traumatic brain injury, long-bone fractures, abdominal trauma and patients requiring mechanical ventilation.
ResultsA total of 376 patients met the inclusion criteria, 220 of whom were males (58.5%). The most frequent causes of trauma were falls (218 cases; 57.9%) and motor vehicle accidents (57 cases; 15.1%). The most frequent type of trauma was rib contusion (248 cases; 65.9%) and rib fractures (61 cases; 16.2%). Complications were observed in 43 patients (11.4%), mainly hemothorax (13 cases), pneumothorax (9 cases), pneumonia (6cases) and acute renal failure (4 cases). Four patients died due to pneumonia and hemothorax. Thirty-three patients were hospitalized (8.7%) and 10 (2.6%) required later re-admittance. The risk for complications increased significantly in patients with more than 2 rib fractures, in those over the age of 85 and in the presence of certain comorbidities, such as COPD and pathologies requiring anticoagulation therapy. The risk for re-admittance is higher in patients over the age of 60.
ConclusionsPatients with chest trauma who present certain comorbidities, are over the age of 85 and have more than 2 rib fractures may present more complications. These factors should be contemplated in the evaluation, management and follow-up of these subjects.
Describir las características clínicas y los factores de riesgo de los pacientes con traumatismo torácico, y evaluar su relación en el desarrollo de complicaciones.
MetodologíaEstudio de tipo descriptivo, prospectivo y analítico de una cohorte de pacientes con traumatismo torácico a los que se les hizo seguimiento durante un periodo de 30días. Se excluyeron pacientes con traumatismo craneoencefálico moderado a severo, fracturas de huesos largos, traumatismo abdominal, y pacientes que requirieron ventilación mecánica.
ResultadosUn total 376pacientes cumplieron criterios de inclusión, y de ellos 220 eran varones (58,5%). Las causas más frecuentes de traumatismo fueron las caídas (218casos; 57,9%) y los accidentes de tráfico (57casos; 15,1%). El tipo de traumatismo más frecuente fue la contusión costal (248casos; 65,9%) y la fractura de un arco costal (61casos; 16,2%). Se observaron complicaciones en 43pacientes (11,4%), principalmente por hemotórax (13casos), neumotórax (9casos), neumonía (6casos) e insuficiencia renal aguda (4casos). De estos pacientes, 4fallecieron por neumonía y hemotórax. Treinta y tres pacientes (8,7%) fueron ingresados y 10 (2,6%) requirieron reingreso hospitalario. El riesgo de complicaciones aumenta significativamente en pacientes con más de 2fracturas costales, en mayores de 85años y en presencia de algunas comorbilidades como la EPOC y patologías que requieren anticoagulación. El riesgo de reingreso es mayor en pacientes con más de 60años.
ConclusionesLos pacientes con traumatismo torácico que presentan algunas comorbilidades, son mayores de 85años y tienen más de2 fracturas costales pueden presentar más complicaciones, y se deben considerar estos factores en su evaluación, manejo y seguimiento.
Injuries are the leading public health problem in the European Union, with a mortality rate of 250000 cases per year.1 Chest trauma is responsible for more than 30% of these deaths, directly or indirectly. However, more than 85% of cases do not require surgery, but rather general measures available to emergency physicians.
Current demographic data show progressive aging of the European population. Spain is not immune to this problem, and in recent years has undergone an increasingly noticeable change in the population pyramid.2 With this increase in the adult population, it is natural that these patients are involved in traumatic accidents.3
Chest trauma is a common problem in our setting; its main causes are motor vehicle, workplace and domestic accidents.4
Epidemiological data published on mild and moderate chest trauma are generally from retrospective studies.5 It is considered that patients with mild chest trauma, with no signs of complications, can be treated on an outpatient basis. However, it should be remembered that in elderly patients, low-energy traumas such as falls can cause serious problems.
There are many publications on moderate-severe chest trauma, or in the context of patients with multiple trauma.5,6
A study was proposed to describe the clinical and demographic characteristics, comorbidities and risk factors of patients with chest trauma, and to follow them up closely to assess their evolution, since patients who initially survive may develop complications in the hours, days and weeks following the trauma, which may even lead to death.7
MethodologyHospital Universitario 12 de Octubre is a tertiary referral hospital for the southern Madrid area and other districts in the region, and for other autonomous regions. It is one of the largest hospitals in Spain, with more than 1300 beds, 34 theaters for elective surgery and 4 for urgent procedures. It takes at least 44000 hospital admissions annually from an estimated population of 412930 persons, distributed in a population pyramid very similar to that of the rest of the country.
The study population was a total of 514 patients (of whom 138 were excluded) who consecutively attended the Emergency Department of our hospital for chest trauma between 1 February and 30 April 2011. Patients with moderate to severe traumatic brain injury (TBI), long-bone fractures, abdominal trauma and patients requiring mechanical ventilation were excluded.
This is a descriptive, prospective and analytical study of a patient cohort. All patients were evaluated in the Emergency department by a Thoracic Surgery resident within the first hour of arrival, following the Advanced Trauma Life Support protocol for the management of chest trauma.8
Based on the clinical and radiological evaluation, they were assigned to outpatient treatment or hospital admission. The criteria for admission were: 3 or more rib fractures and/or the presence of complications such as hemothorax and pneumothorax.
Patients were observed for 30 days following the trauma through the Madrid Community Healthcare System internal information network (HORUS), and followed up at the Thoracic Surgery clinic between the first and second week after the trauma. The following were analyzed: age (as an independent, stratified variable), sex, cause, type (according to radiological involvement) and place where the trauma occurred, presence of comorbidities, development of complications and number of hospital admissions and readmissions, average length of stay of patients admitted and need for surgery.
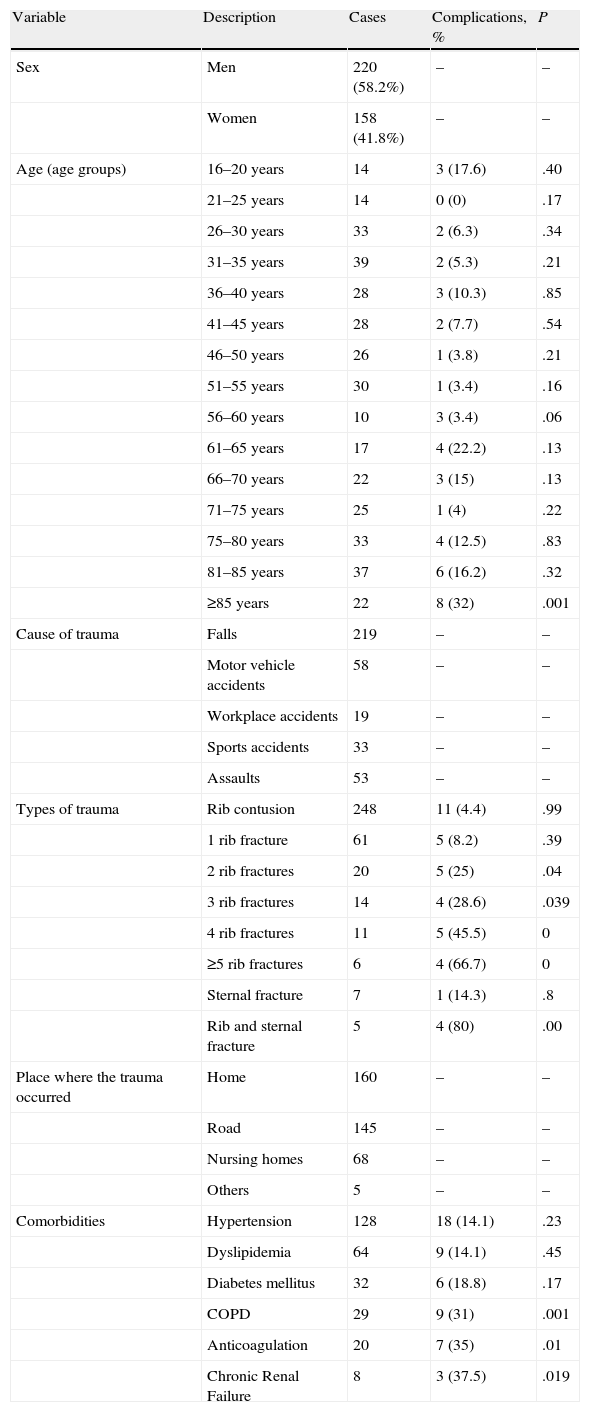
The statistical program used was SPSS 17.0. Univariate analysis was performed to evaluate possible relationships between the development of complications and the other variables studied using the Chi-squared test (Table 1).
Patient Characteristics, Cause and Type of Chest Trauma and Relationship With the Complications Observed.
| Variable | Description | Cases | Complications, % | P |
| Sex | Men | 220 (58.2%) | – | – |
| Women | 158 (41.8%) | – | – | |
| Age (age groups) | 16–20 years | 14 | 3 (17.6) | .40 |
| 21–25 years | 14 | 0 (0) | .17 | |
| 26–30 years | 33 | 2 (6.3) | .34 | |
| 31–35 years | 39 | 2 (5.3) | .21 | |
| 36–40 years | 28 | 3 (10.3) | .85 | |
| 41–45 years | 28 | 2 (7.7) | .54 | |
| 46–50 years | 26 | 1 (3.8) | .21 | |
| 51–55 years | 30 | 1 (3.4) | .16 | |
| 56–60 years | 10 | 3 (3.4) | .06 | |
| 61–65 years | 17 | 4 (22.2) | .13 | |
| 66–70 years | 22 | 3 (15) | .13 | |
| 71–75 years | 25 | 1 (4) | .22 | |
| 75–80 years | 33 | 4 (12.5) | .83 | |
| 81–85 years | 37 | 6 (16.2) | .32 | |
| ≥85 years | 22 | 8 (32) | .001 | |
| Cause of trauma | Falls | 219 | – | – |
| Motor vehicle accidents | 58 | – | – | |
| Workplace accidents | 19 | – | – | |
| Sports accidents | 33 | – | – | |
| Assaults | 53 | – | – | |
| Types of trauma | Rib contusion | 248 | 11 (4.4) | .99 |
| 1 rib fracture | 61 | 5 (8.2) | .39 | |
| 2 rib fractures | 20 | 5 (25) | .04 | |
| 3 rib fractures | 14 | 4 (28.6) | .039 | |
| 4 rib fractures | 11 | 5 (45.5) | 0 | |
| ≥5 rib fractures | 6 | 4 (66.7) | 0 | |
| Sternal fracture | 7 | 1 (14.3) | .8 | |
| Rib and sternal fracture | 5 | 4 (80) | .00 | |
| Place where the trauma occurred | Home | 160 | – | – |
| Road | 145 | – | – | |
| Nursing homes | 68 | – | – | |
| Others | 5 | – | – | |
| Comorbidities | Hypertension | 128 | 18 (14.1) | .23 |
| Dyslipidemia | 64 | 9 (14.1) | .45 | |
| Diabetes mellitus | 32 | 6 (18.8) | .17 | |
| COPD | 29 | 9 (31) | .001 | |
| Anticoagulation | 20 | 7 (35) | .01 | |
| Chronic Renal Failure | 8 | 3 (37.5) | .019 |
Statistical test used: Chi squared test.
Table 1 describes the variables studied and their relationship with the development of the complications observed in the patients in this series.
A total of 376 patients met the inclusion criteria, 220 males (58.2%) and 156 females (41.8%). The age group that most frequently visited the Emergency department was between 31 and 35 years (38 patients; 10.1%), followed by the group between 81 and 85 years (37 patients; 9.8%). The number of complications increased over the age of 60; their relationship was significant over the age of 85, independently of the type of trauma (Table 1).
The most common causes of chest trauma were falls (218 cases; 57.7%) mainly in patients over 71, and motor vehicle accidents (57 cases; 15.1%), predominantly in those aged between 31 and 55 years (Fig. 1).

The most common types of trauma were rib contusion (248 cases; 65.6%) and rib fractures (61 cases; 16.1%). With respect to the development of complications according to the number of rib fractures, the appearance of complications was statistically significant when there were more than 2 rib fractures (Table 1).
The most common accident site was the home (160 cases; 42.5%), road (145 cases; 38.5%) and nursing homes (68 cases; 18.1%).
The comorbidities observed in these patients were: hypertension (HT) (128 cases; 33.9%), dyslipidemia (64 cases; 16.9%), diabetes mellitus (DM) (32 cases; 8.5%), chronic obstructive pulmonary disease (COPD) (29 cases; 77%), pathologies associated with anticoagulation therapy (20 cases; 5.3%) and chronic renal failure (CRF) (8 cases; 2.1%). With respect to the number of comorbidities per patient: 66 patients had one, 101 patients had two, 51 patients three and 6 patients four. The relationships between comorbidities and the development of complications are described in Table 1; COPD, CRF, and pathologies associated with anticoagulation therapy were statistically significant.
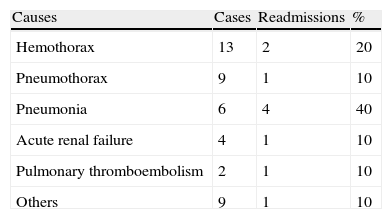
Complications were diagnosed in 43 patients: hemothorax (13 cases; 3.4%), pneumothorax (9 cases; 2.4%), pneumonia (6 cases; 1.5%), and others (anemia, heart failure, respiratory failure, pleural effusion, atelectases). No patient had more than one complication (Table 2).
Fourteen patients had complications on admission. The rest appeared during admission or in the follow-up between the third and fifteenth day, with a mean of 4.58 days.
Thirty-three patients were admitted (8.7%), with an average stay of 4.75 days. Ten patients had to be readmitted (2.6%) (Table 2).
Four patients died due to pneumonia and hemothorax (1.1%).
A total of 20 chest drains were inserted due to hemothorax and pneumothorax. A total of 4 surgeries, 3 thoracotomies, and one video-assisted thoracoscopy (VATS) were performed, all due to persistent hemothorax that did not resolve with drainage.
DiscussionThis study was designed to analyze the characteristics of patients with isolated chest trauma who attended the emergency department of a tertiary hospital, and the relationship of these characteristics with the development of complications. Since all patients who attended the emergency department during the study period were included, this gives a fairly real idea of their characteristics, which may be extrapolable to the rest of the population.
We observed that the main cause of trauma was falls, which differs from that published in other series, where motor vehicle accidents were the main cause of chest trauma5,6; this may be related to the high number of elderly patients in our series.9 Furthermore, by excluding patients with multiple trauma and involvement of other organs, a large number of traumas caused by motor vehicle accidents were excluded, which is one of the limitations of our study.Patients with more than two rib fractures had a significantly higher risk of suffering complications, which does not correspond with the findings of other published series, which report that the number of rib fractures with a statistically significant relationship with the appearance of complications is three.5,10–12
A higher risk of complications was detected in patients over the age of 60. Over the age of 85, the probability of complications is statistically significant, and is also independent of the type of trauma. These data differ from those published in other Spanish series, which report that morbidity does not increase in patients over 70, because they are minor traumas: falls or domestic accidents.5 This may be because follow-ups were not carried out in these series, while in our series, the complications were observed in the two weeks following the trauma. A recent study has described a higher risk of complications in patients aged over 65 years.10
Pleural drainage enables most hemothorax and pneumothorax to be resolved, and avoids surgery in 80% of cases, which confirms its importance and utility in resolving hemothorax and pneumothorax and avoiding surgery.7,10,13
The presence of comorbidities (COPD and CRF),14,15 use of anticoagulants and the presence of rib fractures have a major effect on reducing survival.10,15 We did not observe this effect in our series, but we did note a significant increase in the frequency of complications.
Readmission of patients who have suffered a chest trauma has not been described in other publications, probably because there are few prospective studies in which close follow-up was carried out, as in our series, in which the risk of readmission increased in patients aged over 60. The most common cause was pneumonia and, although this complication has been described in other publications, it was observed during the hospital stay.15,16
The mortality was low, despite the large number of elderly patients. This finding has been described by other authors, who suggest that this is because traumas in elderly patients are mainly due to falls and are low-energy.5,17 However, other series differ from this, and describe high mortality in elderly patients.18,19
In conclusion, the factors indicated above in this series, which may increase complications in chest trauma, should be contemplated in the evaluation, management and follow-up of patients with this injury.
Conflict of InterestsThe authors declare no conflict of interests.
Please cite this article as: Ávila Martínez RJ, et al. Evolución y complicaciones del traumatismo torácico. Arch Bronconeumol. 2013;49:177–80.







