

We report the case of a 58-year-old man with no history of interest, who presented with asthenia, adynamia, drowsiness, and dyslalia. Laryngoscopy showed diffuse and ulcerated transglottal lesions, and carcinoma was suspected. A chest X-ray was performed, which revealed bilateral fibrothorax of undetermined etiology (Fig. 1A). The patient died suddenly from no clearly defined cause. Due to his rapid deterioration and fatal outcome, no serological or immunological studies were possible.
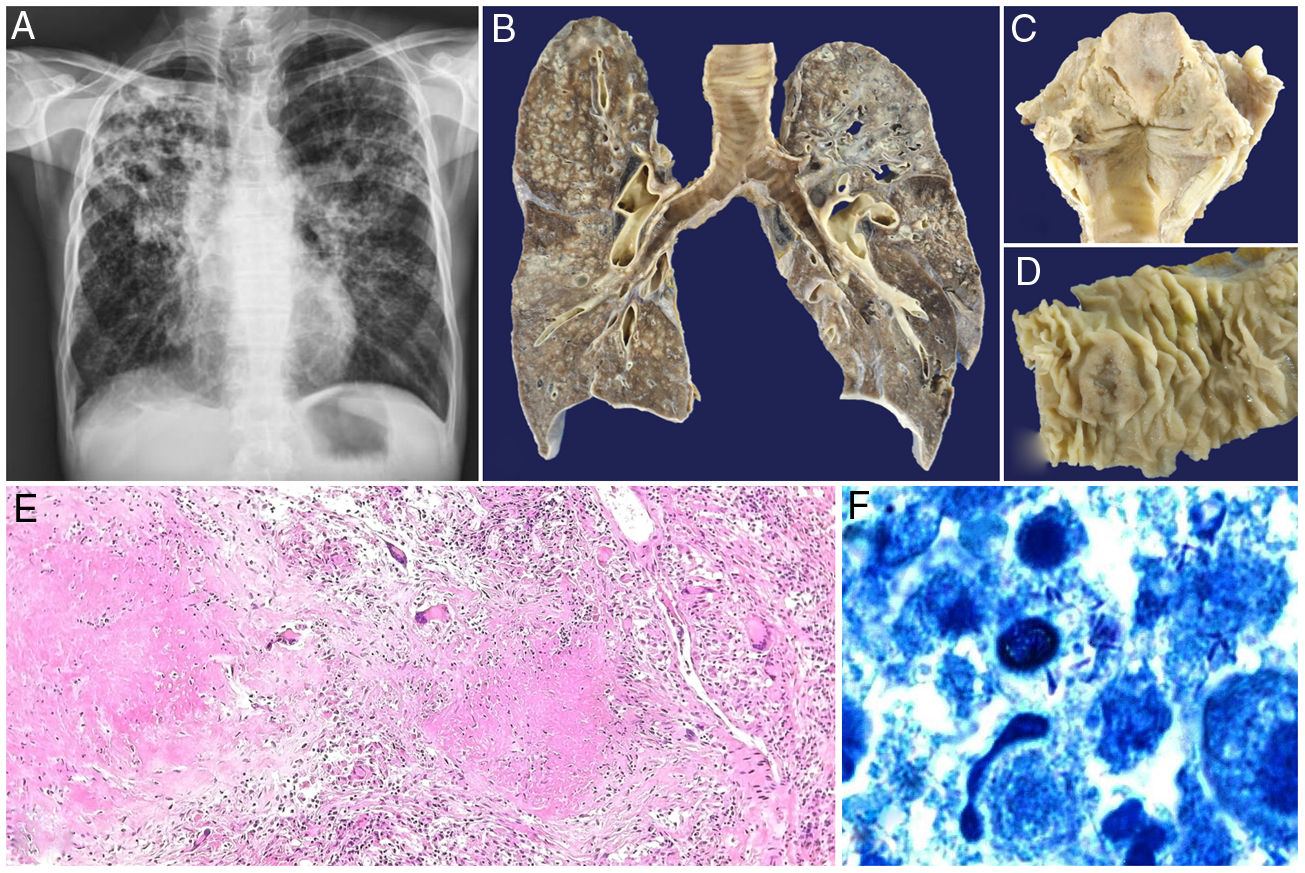
Autopsy revealed pulmonary tuberculosis with histological criteria of activity and acino-nodular, cavitated, and miliary patterns (Fig. 1B) spreading to the larynx, which showed a diffusely ulcerated surface with a crazy-paving appearance (Fig. 1C); in the gastrointestinal tract, oval ulcers were observed perpendicular to the longitudinal axis of the intestine (Fig. 1D), bone marrow, spleen, and mediastinal and mesenteric lymph nodes. Granulomatous inflammation (Fig. 1E) and the presence of acid-alcohol-resistant bacilli were confirmed microscopically with Ziehl-Neelsen staining (Fig. 1F). The patient died due to peritonitis secondary to a perforated ulcer in the ileocecal junction.
The diagnosis of tuberculosis can be challenging, especially in low-incidence regions or in the case of an atypical clinical picture, such as ours, in which laryngeal carcinoma was suspected, but due to the lack of etiological diagnosis and targeted treatment, the outcome was the unexpected death of the patient.1,2
FundingNone declared.
Conflict of interestNone.







