

CURRENT SITUATION AND LONG-TERM CONSEQUENCES OF COVID-19 INFECTION
More infoThe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) disease (COVID-19) pandemic is imposing an unprecedented global burden on Health Systems.1,2 The active participation of Pulmonology specialists in the first-line response against COVID-19 forced a rapid reorganization of hospital departments to manage a high number of contagious patients with variable levels of respiratory failure or other medical COVID-related complications. Scientific communities raised concern regarding the impact of COVID-19 on the global control of the tuberculosis (TB) epidemic because of the weakening of TB programmes and the potential interactions between these two infections.3–6
As the fight against the pandemic continued, Pulmonology Departments continued to manage non-COVID-19 patients, including those with TB implementing some necessary organizational re-structuring.7
We aimed to describe the re-organization of a major Pulmonology Department under the COVID-19 emergency and the main productivity outputs with special focus on diagnosis and admission of TB patients.
The study, retrospective and descriptive, was conducted at the Pulmonology Department of Centro Hospitalar de Vila Nova de Gaia/Espinho (CHVNG/E) (Portugal). The study is part of a larger international initiative of the Global Tuberculosis Network (GTN).7,8
CHVNG/E is a central hospital providing healthcare to a catchment area of 334,000 inhabitants. According to its referral networks, CHVNG/E has assigned a larger influence area of 700,000 inhabitants.9 CHVNG/E is a reference centre for several diseases, including TB, and works in a close relationship with the TB outpatient center (TBOC) of Vila Nova de Gaia/Espinho, which is responsible for the diagnosis, treatment, screening and prevention of all TB cases in the area. Most TB cases are managed on an outpatient basis and only few (severe or drug-resistant) patients are hospitalized.
We collected data from the Hospital Statistics Service and the Clinical Pathology Department on the re-organization procedures and on health services provided (including the total number of clinical appointments at the TBOC and of laboratory TB diagnosis). We conducted an analytical study comparing outpatient activity, overall hospitalizations, bronchoscopy procedures and tuberculosis diagnosis and hospitalizations over the first six months (January–June) of 2019, 2020 and 2021.
COVID-19 led to the quick implementation of nationwide measures to reduce the spread of the SARS-CoV-2 virus and strengthen the capacity of the National Health System. In Portugal, the Emergency State was declared on March 18, 2020 and three COVID-19 waves were subsequently documented: March-early May 2020; early October–December 2020 and December 2020–early February 2021. After the “Portuguese miracle” observed in the first wave, the country faced a dramatic third wave, with one of the world's highest numbers of COVID-19 deaths.10 The Northern region, where the study was performed, suffered very high morbidity and mortality (Portuguese General Health Direction data).11
The CHVNG/E Pulmonology Department offers hospitalization (23 beds in the general ward and 4 beds to patients with acute respiratory failure under noninvasive ventilation) and day hospital services. It includes the following units: outpatient clinic; bronchology; respiratory function laboratory; obstructive lung disease; noninvasive ventilation; respiratory rehabilitation; allergic asthma; thoracic oncology; smoking cessation; sleep respiratory disorder; interstitial lung diseases; lung transplantation and pulmonary hypertension.
As the pandemic intensified, CHVNG/E created many isolation wards exclusively dedicated to inpatients with confirmed COVID-19. Teams devoted to COVID-19 included physicians from almost all medical and surgical specialities available in the hospital.
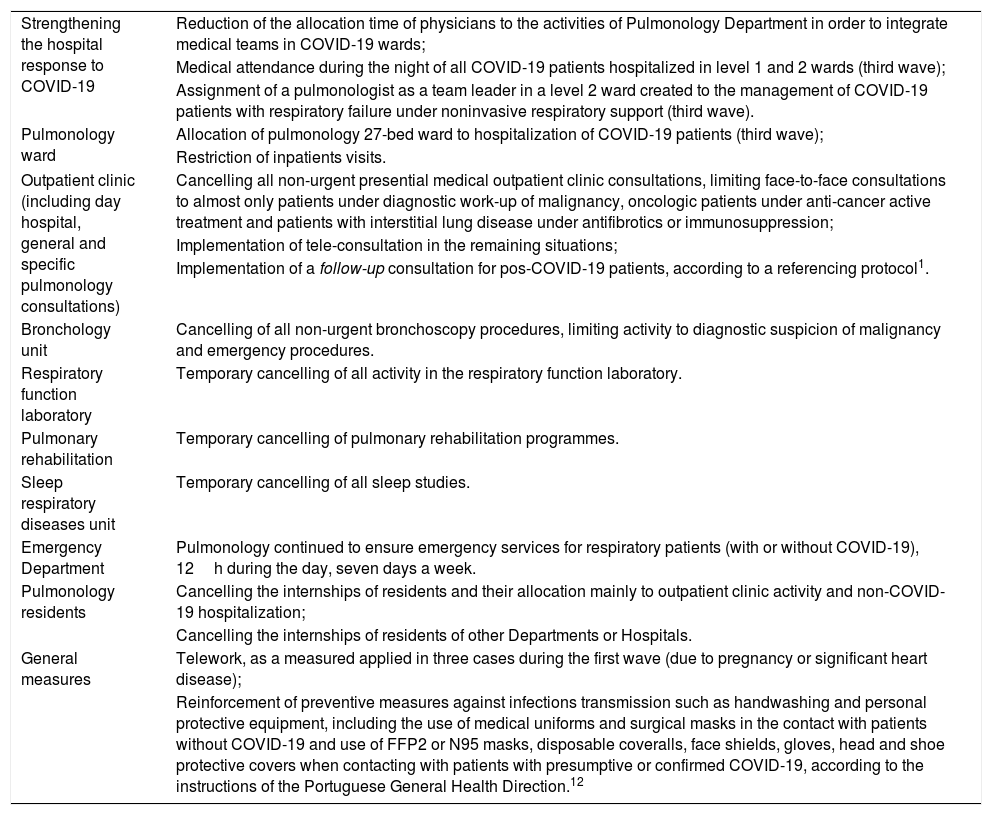
The first wave of COVID-19 forced many organizational changes in the Pulmonology Department (Table 1), reinforced during the second and, especially, the third wave.
Strategies implemented in the CHVNG/E Pulmonology Department in response to COVID-19 pandemic.
| Strengthening the hospital response to COVID-19 | Reduction of the allocation time of physicians to the activities of Pulmonology Department in order to integrate medical teams in COVID-19 wards; |
| Medical attendance during the night of all COVID-19 patients hospitalized in level 1 and 2 wards (third wave); | |
| Assignment of a pulmonologist as a team leader in a level 2 ward created to the management of COVID-19 patients with respiratory failure under noninvasive respiratory support (third wave). | |
| Pulmonology ward | Allocation of pulmonology 27-bed ward to hospitalization of COVID-19 patients (third wave); |
| Restriction of inpatients visits. | |
| Outpatient clinic (including day hospital, general and specific pulmonology consultations) | Cancelling all non-urgent presential medical outpatient clinic consultations, limiting face-to-face consultations to almost only patients under diagnostic work-up of malignancy, oncologic patients under anti-cancer active treatment and patients with interstitial lung disease under antifibrotics or immunosuppression; |
| Implementation of tele-consultation in the remaining situations; | |
| Implementation of a follow-up consultation for pos-COVID-19 patients, according to a referencing protocol1. | |
| Bronchology unit | Cancelling of all non-urgent bronchoscopy procedures, limiting activity to diagnostic suspicion of malignancy and emergency procedures. |
| Respiratory function laboratory | Temporary cancelling of all activity in the respiratory function laboratory. |
| Pulmonary rehabilitation | Temporary cancelling of pulmonary rehabilitation programmes. |
| Sleep respiratory diseases unit | Temporary cancelling of all sleep studies. |
| Emergency Department | Pulmonology continued to ensure emergency services for respiratory patients (with or without COVID-19), 12h during the day, seven days a week. |
| Pulmonology residents | Cancelling the internships of residents and their allocation mainly to outpatient clinic activity and non-COVID-19 hospitalization; |
| Cancelling the internships of residents of other Departments or Hospitals. | |
| General measures | Telework, as a measured applied in three cases during the first wave (due to pregnancy or significant heart disease); |
| Reinforcement of preventive measures against infections transmission such as handwashing and personal protective equipment, including the use of medical uniforms and surgical masks in the contact with patients without COVID-19 and use of FFP2 or N95 masks, disposable coveralls, face shields, gloves, head and shoe protective covers when contacting with patients with presumptive or confirmed COVID-19, according to the instructions of the Portuguese General Health Direction.12 |
CHVNG/E: Centro Hospitalar de Vila Nova de Gaia/Espinho; COVID-19: Coronavirus Disease 2019.
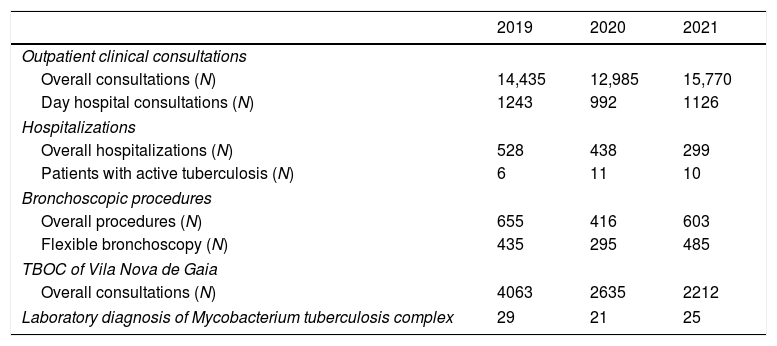
Over the first semesters of 2019 and 2020, we found a predictable decrease in all sectors of activity (Table 2): overall outpatient consultations (17.1%), day hospital (20.2%), hospitalizations (17.1%), bronchoscopy procedures (36.5%) and TBOC consultations (35.1%). Furthermore, other factors may have contributed to this reduction, such as a change in health-seeking behaviour. Patients may have reduced demand for health care because of the fear of COVID-19, not reporting anymore to the emergency department in case of mild or moderate symptoms, and physical constraints resulting from stay-at-home orders.5,13
Activity of Pulmonology Department, TBOC of Vila Nova de Gaia and laboratory diagnosis of Mycobacterium tuberculosis complex in CHVNG/E in the first six months of 2019, 2020 and 2021.
| 2019 | 2020 | 2021 | |
|---|---|---|---|
| Outpatient clinical consultations | |||
| Overall consultations (N) | 14,435 | 12,985 | 15,770 |
| Day hospital consultations (N) | 1243 | 992 | 1126 |
| Hospitalizations | |||
| Overall hospitalizations (N) | 528 | 438 | 299 |
| Patients with active tuberculosis (N) | 6 | 11 | 10 |
| Bronchoscopic procedures | |||
| Overall procedures (N) | 655 | 416 | 603 |
| Flexible bronchoscopy (N) | 435 | 295 | 485 |
| TBOC of Vila Nova de Gaia | |||
| Overall consultations (N) | 4063 | 2635 | 2212 |
| Laboratory diagnosis of Mycobacterium tuberculosis complex | 29 | 21 | 25 |
N: number; TBOC: tuberculosis outpatient centre; CHVNG/E: Centro Hospitalar de Vila Nova de Gaia/Espinho; N: sample size.
The decrease in hospitalizations is in line with a previous study documenting a 57% reduction in hospitalizations in Portugal from March to May 2020.14 According to the same study, more than half of all COVID-19-confirmed cases and hospitalizations occurred in the Northern region (60.0%), revealing the pressure on these hospitals.14
A reduction in laboratory identification of Mycobacterium tuberculosis complex was also documented (27.6%) in the first semester of 2020, which could be explained by the fact that physicians may have been more focused on diagnosing SARS-CoV-2, neglecting other etiologies of respiratory infection, including TB. Moreover, lockdown and personal protective equipment could positively impact TB control by helping mitigate community transmission.15
Over the first semesters of 2020 and 2021, we found an increase in outpatient clinic consultations (21.4%) and bronchoscopy procedures (45.0%), likely reflecting an attempt to recover previous clinical productivity and compensate for the diagnostic and therapeutic delay of other respiratory diseases.16 The increase in Day Hospital consultations could result from different reasons, including referral of post-COVID-19 patients according to a protocol1 guiding early reassessment of some of them (particularly those with signs of interstitial lung disease during the acute phase of COVID-19) or need of oxygen therapy at hospital discharge.
Conversely, a downward in the number of overall hospitalizations (31.7%) and consultations at the TBOC (16.1%) was documented over the first semesters of 2020 and 2021. TBOC recently described the maintenance of its activity, without significant delays between symptoms, diagnosis and treatment, despite the restrictions imposed.17 Patients requiring hospitalization are referred to TBOC at discharge, where treatment and follow-up are assured. Despite the progressive reduction of overall hospitalizations since the beginning of the pandemic, we found a growing trend in the number of TB inpatients (n=6, 2019; n=11, 2020; n=10, 2021), which could suggest an increase in the severity of new cases of TB. This hypothesis is further supported by the observation of a trend towards a reduction in the number of new laboratory TB diagnoses in 2020 (n=21) and 2021 (n=25) compared to the homologous pre-pandemic period (n=29). The finding suggests that, despite the diagnosis of a smaller number of patients, those who are identified present more severe disease. However, among TB hospitalized cases, only one patient had previously presented COVID-19 (mild disease). Among patients with laboratory diagnosis of TB, the extrapulmonary involvement remained approximately constant in the three analyzed periods: 34.5%, 33.3% and 32.0%, respectively. Among all TB patients, only one case of multidrug-resistant TB was reported.
One of the goals of this study was to warn about the need of restructuring of Pulmonology Departments in response to COVID-19 pandemic. At the same time, it intended to show the trends in TB diagnosis and hospitalizations in three homologous periods corresponding to before, during and after the onset of the pandemic. One limitation of this study lies in the reduced number of TB patients throughout the three periods, which might be explained by the fact that only the first six months of each year were analyzed because of methodological reasons.
In conclusion, health resources were allocated to the COVID-19 needs with an effect on the clinical response to other diseases. Our data reveals the effect of the pandemic on the overall clinical activity and the effort to recover in 2021. Although hospitalization for problems other than COVID-19 decreased, tuberculosis was an exception, despite the observed reduction of new diagnoses (likely related to increased severity as the prevalence of drug resistance did not increase).
Authors’ contributionsAdelaide Alves and Raquel Duarte formulated the initial research questions and study methodology. Ana Aguiar contributed to refining the research and study methodology. G.B. Migliori critically revised the content and drafted some parts of the manuscript. Adelaide Alves was responsible for data analysis. All authors were involved in data interpretation. Adelaide Alves wrote the first draft of the paper. Ana Aguiar and Raquel Duarte reviewed the document. All authors provided inputs on and approved the final version of the manuscript.
FundingNo specific funding was received for this work. However, Ana Aguiar holds a PhD Grant (2020.09390.BD), cofunded by the Fundação para a Ciência e a Tecnologia (FCT) and the Fundo Social Europeu (FSE) Program.
The project is supported scientifically by the Global Tuberculosis Network (GTN).
This article belongs to the scientific activities of the WHO Collaborating Centre for Tuberculosis and Lung Diseases, Tradate, ITA-80, 2010-2024-GBM/RC/LDA.
The authors wish to thank Rosella Centis (Istituti Clinici Scientifici Maugeri, Tradate, Italy) and Lia D’Ambrosio (Public Health Consulting Group, Lugano, Switzerland) for the editorial support.
Conflict of interestThe authors declare to have no conflict of interest directly or indirectly related to the manuscript contents.







