

The nature of human beings and the societal structure of our lives sometimes offer infectious diseases an opportunity to disseminate beyond our control. This is of particular importance when diseases develop into epidemics or pandemics, and at such times scientific innovations combined with social transformations are often necessary.
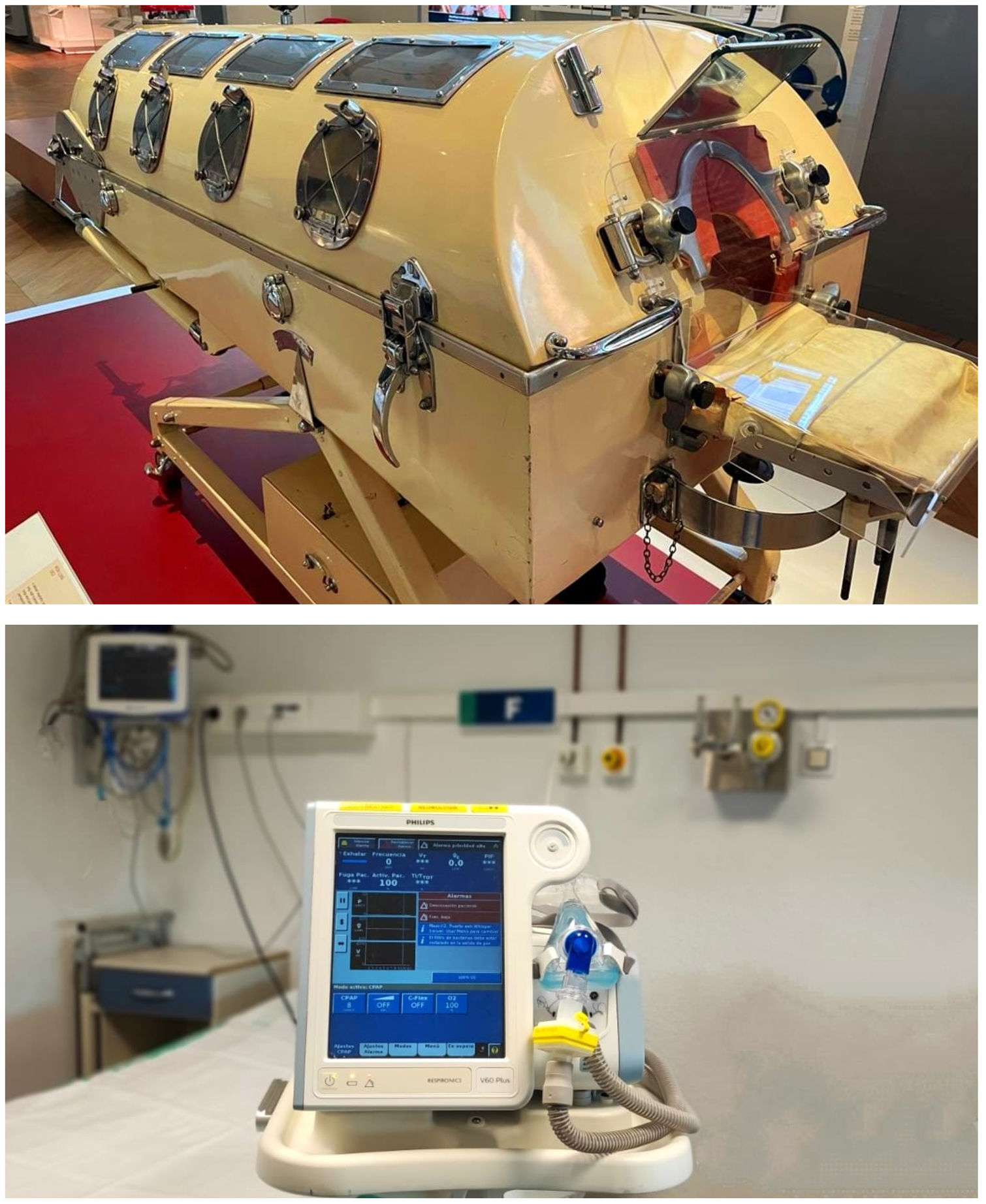
In both the poliomyelitis epidemic in the first half of the 20th century and the COVID-19 pandemic, non-invasive respiratory support (NIRS) became the savior of many patients who would otherwise have suffered respiratory failure and eventually death. The iron lung, developed by Drinker-Shaw in 1928, was the first negative-pressure electric ventilator to achieve widespread success in clinical practice.1 The equipment was subsequently enhanced by Emerson, and went on to become the cornerstone of treatment in patients with respiratory paralysis due to polio, until positive pressure ventilation was reintroduced in the 1950s.2 Every polio epidemic generated investment in technology aimed at improving existing ventilators, and thousands of lives were saved around the world. This long history of therapeutic advances has now helped respiratory experts confront one of the most important pandemics of the 21st century (Fig. 1).
Although COVID-19 is mild or uncomplicated in most patients, approximately 15%3 develop severe disease that may involve acute respiratory distress syndrome (ARDS) that requires admission to an intensive care unit (ICU) for intubation and invasive ventilation. The exponential increase in hospitalizations and the lack of know-how in the management of the disease and essential protective measures initially overwhelmed these units during the early stages of the pandemic. Until that point, the use of NIRS during viral pandemics was controversial, since this intervention was only indicated in the literature for hypercapnic respiratory failure and/or acute pulmonary edema.4 Nevertheless, respiratory experts quickly pooled their accumulated experience and reacted rapidly to manage the limited resources available, coming up with the best possible approach for dealing with this unprecedented epidemiological challenge. As scientific updates emerged worldwide, the Spanish Society of Pulmonology and Thoracic Surgery (SEPAR) worked alongside another 3 Spanish scientific societies specialized in the management of critical respiratory patients to develop a consensus document on NIRS in adults with COVID-19 acute respiratory failure (ARF).5 These recommendations not only helped clinicians to identify patients with ARF who would be candidates for NIRS and select the most appropriate support strategy, but also established measures for prevention and control of infection in patients undergoing these therapies, thus optimizing care and signposting the way for future lines of COVID-19 research.
Another development during the initial waves of the pandemic was the proliferation of intermediate respiratory care units (IRCUs). These units flourished in response to the urgent need to treat and monitor patients with severe ARF who were not ill enough to require ICU admission or for whom a ceiling of treatment had been established (step-up model), and to provide specialist areas where patients discharged prematurely from the ICU (step-down) could continue their treatment. Before the pandemic, 16 of these units existed in Spain. By the end, there were 41, and the capacity of all had significantly increased.6 Their resources also needed an overhaul, and advanced NIRS equipment and monitoring devices, together with ultrasound, bronchoscopy and transcutaneous CO2 systems, were brought in. The nurse/patient ratio had to be increased from pre-pandemic levels and more physicians working shifts of at least 12h were needed to ensure the care and safety of semicritical patients admitted to the IRCUs.7 Physiotherapists, who play a fundamental part both in the control of secretions and the early recovery of the locomotor system, were recruited. This restructuring and capacity for change helped us respond to the immense burden of care while continuing to offer quality care despite the complicated epidemiological framework.
Based on evidence accumulated during the pandemic, the phenotypes of COVID-19 patients with ARF have been defined and the most appropriate treatment strategies have been determined, including when to replace conventional oxygen therapy with NIRS, what type of therapy to select, the role of combined methods, definitions, attitudes toward treatment failure, and better case improvement procedures.8 Refinements in the logistical and structural organization have made our respiratory medicine departments, and more specifically our IRCUs, more effective, as became patent during the pandemic.9 Furthermore, the technical knowledge of our respiratory specialists in the management of NIRS has been acknowledged.
It seems clear, then, that all hospitals in Spain need an IRCU, and this awareness has prompted SEPAR to devote 2022 to raising the visibility of these units.10 COVID-19 is a disease that is at risk of becoming endemic, yet COVID-19 ARDS is by no means the only manifestation presented by critical respiratory patients. Now that IRCUs have demonstrated their value and efficacy, and specialist respiratory departments have proven their ability to lead and adapt, we must maintain the structure of these units for both epidemiological emergencies and normal times. Thus, our aim is to treat any semicritical respiratory patient who may benefit from admission and care in these units, avoiding more aggressive, costly or otherwise counterproductive measures. An IRCU in every hospital is an initiative that aims to provide equitable care throughout Spain, ensuring that a person's postcode does not determine access an IRCU.
FundingThe authors of this editorial have received no specific grants from public sector agencies, the industry, or non-profit organizations for writing this manuscript.
Conflict of interestsNone declared.
We thank David Díaz-Pérez for his permission to use the photograph that appears in the upper half of Figure 1.
The following are the supplementary data to this article:








