


Spontaneous pneumothorax is a disease with an incidence of 7.4–18 cases/100000 inhabitants/year in males and 1.2–6 cases/100000 in females. In the majority of cases, its pathogenesis is associated with bullae, blebs, and subpleural emphysema. There is also a known association between emphysematous pulmonary bullae and lung cancer, but this neoplasm very rarely predisposes to the appearance of a pneumothorax as the initial clinical manifestation – 0.03% being the incidence due to lung tumour disease – and its association with pulmonary metastases is even more rare.1
We present a case of pneumothorax in a patient with pulmonary metastases from a medullary thyroid carcinoma that was discovered during surgical intervention to treat the pneumothorax.
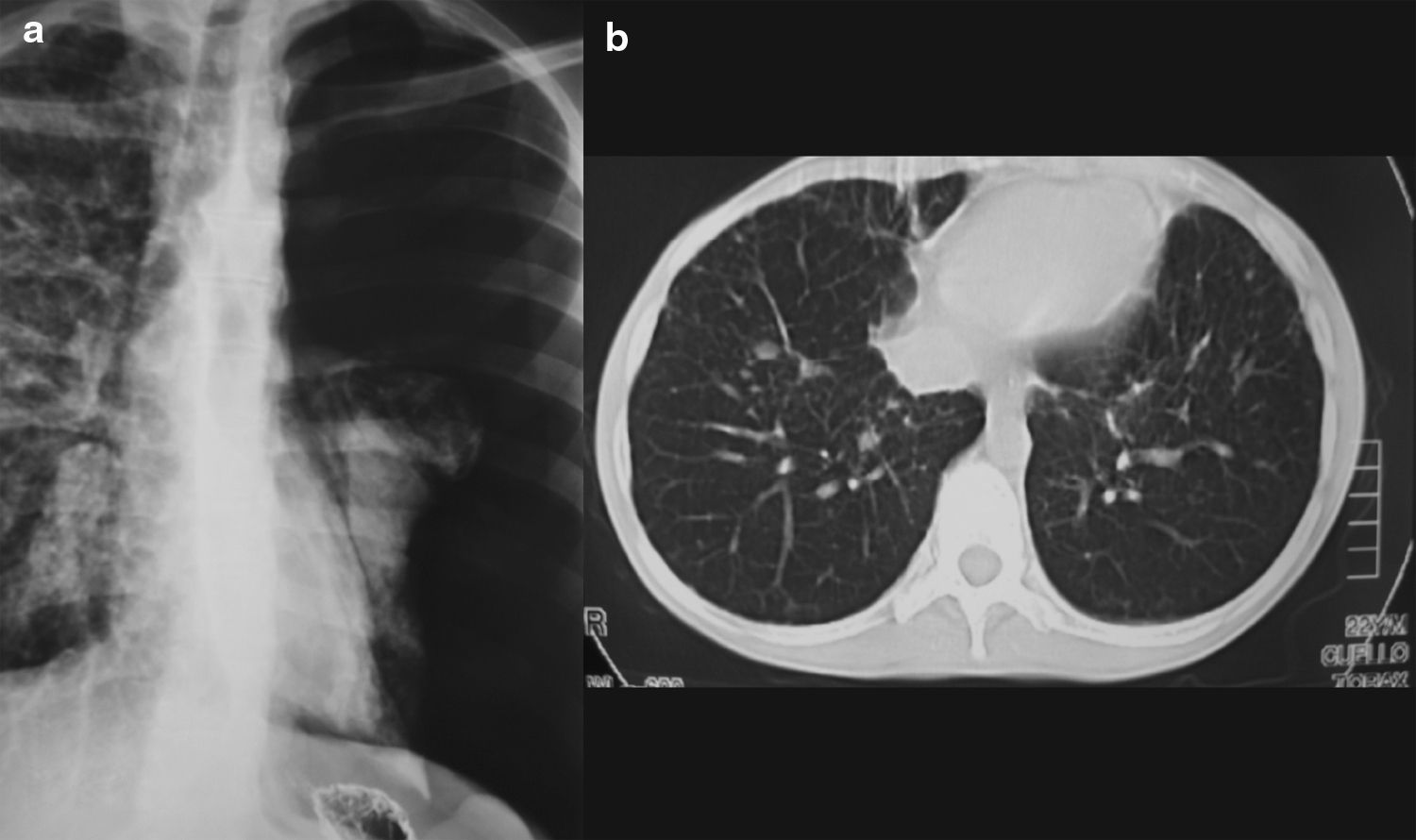
Patient was a 21-year-old male, height 191cm and weight 55kg, with a history of intestinal malabsorption syndrome, who was undergoing workup for clinical suspicion of Marfan syndrome. In the course of a gastrointestinal barium X-ray study, patient reported pain in the left hemithorax. Upon physical examination, diminished breath sounds were noted over the left hemithorax. Chest X-ray showed a left spontaneous pneumothorax. At 24h, patient underwent videothoracoscopy, in which the parenchyma was noted to be dystrophic in appearance, with whitish micronodules across the entire lung surface. In view of these intra-operative findings, a biopsy was taken of the upper and lower lobes of the lung for anatomical pathology study of the nodules.
The biopsy was reported as metastasis of a neuroendocrine carcinoma, probably medullary thyroid carcinoma. Thyroid scan, computerized tomography (CT), and cervical ultrasound confirmed a thyroid tumour with jugular-carotid and submental adenopathies. Likewise, the chest CT scan showed numerous pulmonary nodules suggestive of pulmonary metastases, of various sizes but not larger than 1cm (Fig. 1).
 Posterior–anterior chest X-ray taken during gastrointestinal barium study. (b) Computerized tomography where micronodular pattern is seen in the pulmonary parenchyma.")
Patient underwent a total thyroidectomy, which confirmed a medullary thyroid carcinoma, and was referred for adjuvant oncological therapy.
The appearance of spontaneous pneumothorax in pulmonary neoplasm, whether primary or metastatic, is quite rare. In this type of patient, the cause of the pneumothorax is related to rapid growth of the tumour. This means that, from an oncological standpoint, the prognosis is poor because the disease is already at an advanced stage when it is diagnosed. There are different theories associating pneumothorax with pulmonary metastases. One theory is that it may be related to tumour necrosis2—rupture of a tumour nodule due to necrosis or the necrosis of a subpleural metastasis may cause communication between the bronchioles and the pleural cavity, resulting in a pneumothorax.3 Other theories4 point towards the valvular mechanism by which peripheral tumour nodules may obstruct bronchiolar structures and cause distension due to increased pressure in the already-weakened parenchyma, giving rise to bullae and, when they rupture, a pneumothorax. Lastly, Chen et al.5 associate pneumothorax caused by tumour emboli with distant necrosis. Pneumothorax caused by pulmonary metastases appears frequently in osteosarcoma, with a 5%–7% incidence, but it has also been reported in other sarcomatous tumours and in other tumours following adjuvant therapy.5 In the medical literature, however, there are very few cases of pneumothorax due to pulmonary metastases of thyroid cancer.6
Please cite this article as: Moreno Merino S, et al. Neumotórax espontáneo como primera manifestación de carcinoma medular de tiroides. Arch Bronconeumol. 2011;47:615–6.







