


We would like to congratulate Dr. Ramos et al.1 for their interesting description of elastofibroma dorsi (ED). In their study, these authors concluded that this entity is a tumor of the chest wall that is not sufficiently diagnosed, whose influence is uncertain and whose surgical resection is only indicated in symptomatic patients. We would like to provide and describe our experience with a similar case, including the findings of the magnetic resonance, giving special attention to the diffusion-weighted images.
Elastofibroma is a benign fibroblastic tumor that is almost always located in the lower subscapular region between the scapula and the chest wall. This type of tumor has been detected by coincidence in up to 2% of senior patients by means of computed tomography (CT).2 ED is a recognized process in published anatomopathologic studies and has been receiving attention in recently-published radiological studies because captation of fluorodeoxyglucose (FDG) is frequently observed in these tumors with positron emission tomography (PET)/CT.3–5 We report a case of ED in which magnetic resonance (MR) showed intense diffusion restriction, which should not be mistakenly interpreted as the anomalous restriction that is observed in malignant lesions.
The patient is a 41-year-old woman with diagnosis of thymic carcinoma, treated with chemotherapy and radiotherapy. Chest CT showed an anterior mediastinal mass that did not modify after treatment. Later, the patient underwent thoracic MR that showed no signs of activity of the mediastinal mass with either contrast or diffusion restriction. Another mass was observed, however, in the right lower subscapular region between the scapula and the chest wall. The mass was associated with a low intensity signal in T1 and T2 and a moderately heterogeneous and intense restriction in the diffusion-weighted sequences (Fig. 1). The mass was stable when compared with previous exams. The histopathologic exam demonstrated striations of fatty tissue that alternated with fibrous tissue. The hypertrophic fibrous tissue contained fibrillar material with staining identical to the necrotic fibrous tissue, muscle and fat. These findings were compatible with ED.
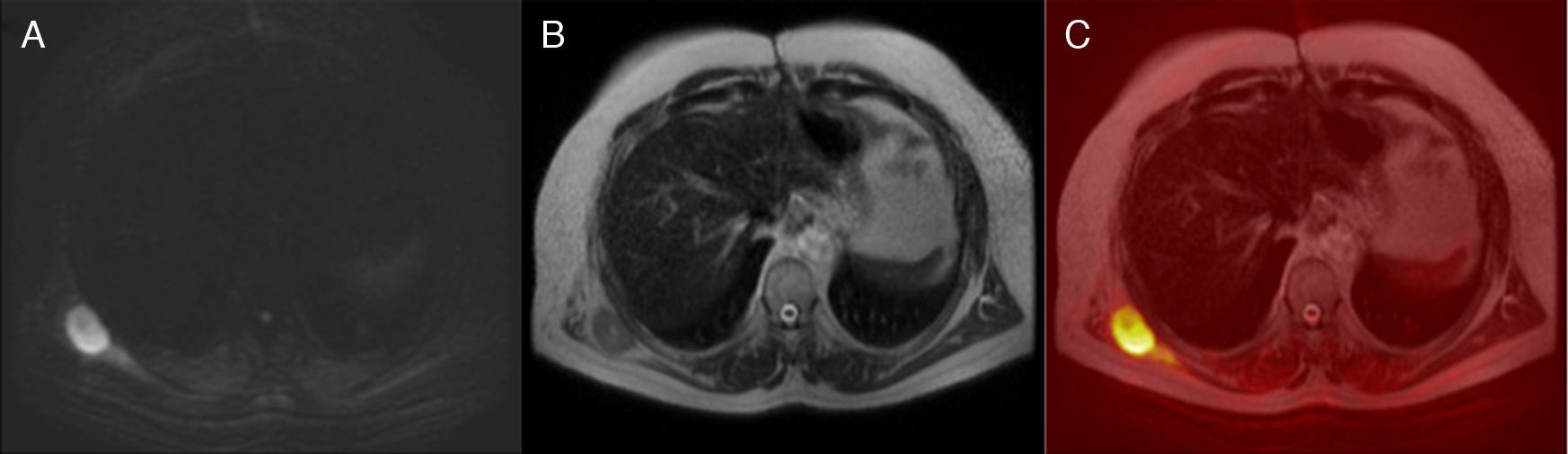
 Diffusion-weighted sequence (b value=600) showing a mass with intense restriction in the right lower subscapular region between the scapula and the chest wall. (B) The mass is characterized by a moderately heterogeneous isointense signal in T2. (C) The fusion of the diffusion-weighted sequence in T2 demonstrates more clearly the intense restriction in the mass.")
(A) Diffusion-weighted sequence (b value=600) showing a mass with intense restriction in the right lower subscapular region between the scapula and the chest wall. (B) The mass is characterized by a moderately heterogeneous isointense signal in T2. (C) The fusion of the diffusion-weighted sequence in T2 demonstrates more clearly the intense restriction in the mass.
Recently, published clinical cases have documented the coincidental detection of an ED with PET/CT. In these cases, mild or moderate captation of FDG was frequently observed, which should not be mistakenly interpreted as the anomalous accumulation of malignant lesions.3–5 Diffusion-weighted MR was also used to evaluate the malignant lesions but, to date, no findings of ED have been described with these sequences. Diffusion-weighted MR images provide functional information (meaning the diffusivity of water molecules) and can highlight high cellularity lesions throughout the body. Diffusion-weighted sequences can be a powerful addition to anatomical MR, detecting subtle lesions and pathological changes in structures in normal size, while reducing the time for interpretation of the images.6 In conclusion, we have observed diffusion restriction on MR in a patient with ED, which could be associated with the inflammatory process of this benign lesion. This finding should not be mistakenly diagnosed as a malignant tumor.
Please cite this article as: Hochhegger B, et al. Imágenes de resonancia magnética ponderadas en difusión en el elastofibroma dorsi. Arch Bronconeumol. 2011. doi:10.1016/j.arbres.2011.06.006.







