


The interesting editorial by Martínez-González1 on changes in the clinical and epidemiological profile of pneumoconiosis caused by exposure to silica in our country highlights a novel source of exposure: the emergence in the 1990s of artificial quartz agglomerates (AQA) for the construction of kitchen worktops and surfaces.
In the Spanish province of Cadiz between 2009 and 2012, we detected a cluster of cases in small family decorative stone-working businesses in local industrial parks, where exposed workers specializing in the machine-working of AQA were employed in poor working conditions. In our experience, this emerging silicosis affects young men after intense exposure over short periods of time.2,3
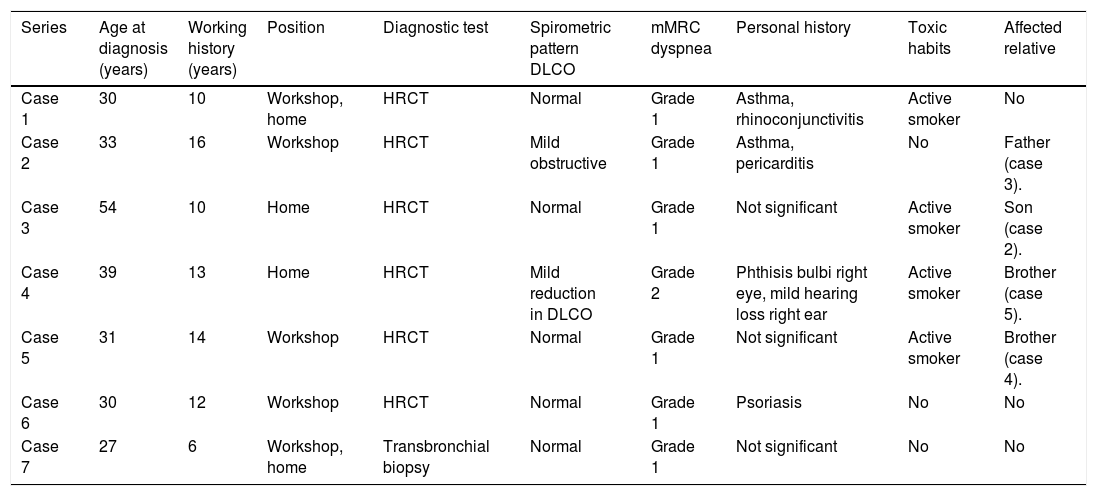
Despite awareness of the danger of this exposure, deficiencies in health and safety measures continue to be detected. As an example, we present the clinical and occupational characteristics (Table 1) of a new cluster of 7 cases diagnosed with simple chronic silicosis at the end of 2015, originating in a decorative stone-working company in Seville employing 11 workers. Mean age at diagnosis was 34.9 years, mean employment history in the company was 11.6 years, and the prevalence of silicosis was 63.6%. Dry polishing, cutting and finishing were carried out in the workshop and in homes, and these finishing activities continued to be performed using dry techniques, despite introducing machinery with water intake in 2011. It is interesting to note the family relationships between 4 of those affected.
Clinical and occupational characteristics of workers.
| Series | Age at diagnosis (years) | Working history (years) | Position | Diagnostic test | Spirometric pattern DLCO | mMRC dyspnea | Personal history | Toxic habits | Affected relative |
|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 30 | 10 | Workshop, home | HRCT | Normal | Grade 1 | Asthma, rhinoconjunctivitis | Active smoker | No |
| Case 2 | 33 | 16 | Workshop | HRCT | Mild obstructive | Grade 1 | Asthma, pericarditis | No | Father (case 3). |
| Case 3 | 54 | 10 | Home | HRCT | Normal | Grade 1 | Not significant | Active smoker | Son (case 2). |
| Case 4 | 39 | 13 | Home | HRCT | Mild reduction in DLCO | Grade 2 | Phthisis bulbi right eye, mild hearing loss right ear | Active smoker | Brother (case 5). |
| Case 5 | 31 | 14 | Workshop | HRCT | Normal | Grade 1 | Not significant | Active smoker | Brother (case 4). |
| Case 6 | 30 | 12 | Workshop | HRCT | Normal | Grade 1 | Psoriasis | No | No |
| Case 7 | 27 | 6 | Workshop, home | Transbronchial biopsy | Normal | Grade 1 | Not significant | No | No |
DLCO: diffusing capacity of carbon monoxide; mMRC: Modified Medical Research Council dyspnea scale; HRCT: high-resolution computed tomography.
Six of the silicosis cases were diagnosed using high-resolution computed tomography (HRCT), and the seventh was diagnosed by transbronchial biopsy after a history of occupational exposure was collected. No standard chest X-rays were performed in examinations conducted before diagnosis. In our practice, the health monitoring of exposed workers must include a standard chest X-ray, although HRCT is useful if the radiological findings are unclear, and for monitoring slow-progressing disease.4 However, confirmatory diagnostic criteria in the management of radiological tests must be fulfilled.
With regard to prevention, doubts have been raised as to the effectiveness of daily exposure limits. In 2015, the National Institute for Health and Safety at Work decreased the limit for free crystalline silica exposure from 0.1mg/m3 to 0.05mg/m3, but the institutions involved must be aware that this reduction in daily exposure limits must also be accompanied by greater rigor in the implementation of both preventive measures and inspections.
Due to the seriousness of the situation in Andalusia (between 2007 and 2015, 126 cases of occupational disease due to silicosis in workers exposed to AQA were reported), a comprehensive pioneer program for this new form of silicosis was proposed in 2017, that is still pending evaluation.5
Although the economic crisis resulted in a decline in the construction sector and consequently in the manufacture and installation of AQA worktops, a resurgence of this economic activity has been observed, so surveillance and monitoring of this emergent form of silicosis must be stepped up, in order to ensure safe and healthy workplaces and to protect workers and their families after diagnosis.
Conflicts of interestThe authors declare no conflicts of interest.
Please cite this article as: Pérez-Alonso A, Córdoba-Doña JA, León-Jiménez A. Silicosis por aglomerados artificiales de cuarzo: claves para controlar una enfermedad emergente. Arch Bronconeumol. 2019;55:394–395.







