


We report the case of a 74-year-old man with lung adenocarcinoma (pT1aN0M0) in the right upper lobe (RUL), treated by segmental resection and post-surgical radiation therapy (RT). Local tumor recurrence was detected during follow-up. Given his high comorbidity, CT-guided microwave thermal ablation (MTA) was administered. The procedure went smoothly and the patient was discharged. However, 1 week later, he attended the emergency room, reporting an oppressive sensation and respiratory distress. On examination, he was eupneic and stable, with crepitation of the soft tissues of the chest and bitonal dysphonia. A chest X-ray revealed marked subcutaneous emphysema, with no signs of pneumothorax (Fig. 1A). Chest CT showed pulmonary cavitation at the MTA site communicating with a bronchus leading to the RUL and with a large gas-filled space in the chest wall, along with extensive pneumomediastinum and subcutaneous emphysema (Fig. 1B–D), findings consistent with bronchial fistula (BF) and bronchocutaneous fistula (BCF) from the post-MTA cavity. The patient was hospitalized and kept under observation and the emphysema was drained. Progress was favorable.
. Extensive subcutaneous emphysema in right chest wall and supraclavicular and cervical region, along with pneumomediastinum (arrows). Poorly delimited mass in the right upper lobe (asterisk), apparently communicating with a bronchus leading to that lobe (arrowheads). Chest CT without intravenous contrast medium, pulmonary parenchyma window. Multiplanar reconstructions in coronal (B) and axial (C) planes, with minimum intensity projection (D). The air cavity is clearly seen surrounding the treated mass (arrowheads in B and C), communicating with a bronchial branch to that lobe (arrowheads in D), along with pneumomediastinum (white arrows) and extensive subcutaneous emphysema predominantly in the right chest wall. Note the large gas-filled space in the chest wall adjacent to the post-thermal ablation cavity, suggesting communication between the two cavities (C and D asterisk). There are also signs of centrilobular emphysema predominantly in the upper lobes.")
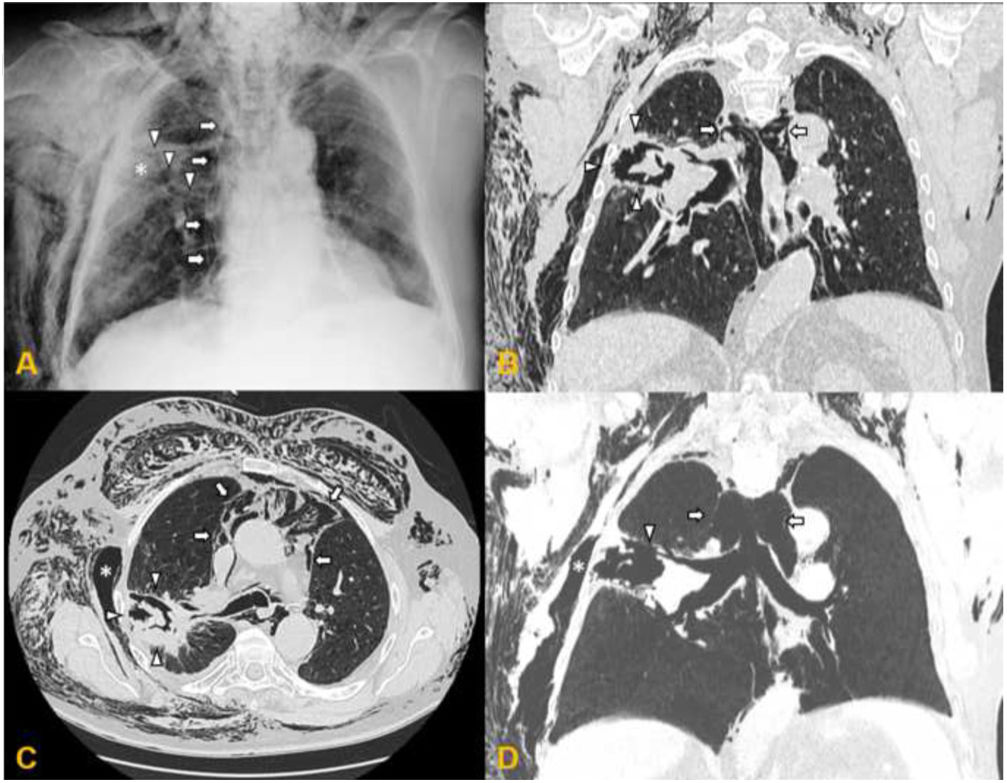
Chest X-ray, PA projection (A). Extensive subcutaneous emphysema in right chest wall and supraclavicular and cervical region, along with pneumomediastinum (arrows). Poorly delimited mass in the right upper lobe (asterisk), apparently communicating with a bronchus leading to that lobe (arrowheads). Chest CT without intravenous contrast medium, pulmonary parenchyma window. Multiplanar reconstructions in coronal (B) and axial (C) planes, with minimum intensity projection (D). The air cavity is clearly seen surrounding the treated mass (arrowheads in B and C), communicating with a bronchial branch to that lobe (arrowheads in D), along with pneumomediastinum (white arrows) and extensive subcutaneous emphysema predominantly in the right chest wall. Note the large gas-filled space in the chest wall adjacent to the post-thermal ablation cavity, suggesting communication between the two cavities (C and D asterisk). There are also signs of centrilobular emphysema predominantly in the upper lobes.
BF and BCF are rare complications of pulmonary thermal ablation (0.4%).1 BFs are usually associated with pneumothorax, although 4 cases of BFs without pneumothorax after thermal ablation have been published, 2 of which occurred after MTA. The proposed mechanism is adhesion between the visceral and the parietal pleura due to excessive MTA energy levels and pleural weakness due to prior RT and surgery.2 Although uncommon, this possible complication of TM must be taken into consideration and the risk-benefit balance should be evaluated according to the patient’s clinical situation.
FundingThis paper has not received any funding.
Conflict of interestsThe authors state that they have no conflict of interests.
Please cite this article as: Láinez Ramos-Bossini AJ, Ruiz Carazo E, López Milena G. Doble fístula tras cavitación de adenocarcinoma pulmonar tratado mediante termoablación con microondas. Una complicación muy infrecuente. Arch Bronconeumol. 2021;57:546.







