






Spain is one of the countries with the highest number of COVID-19 patients. Unfortunately, few data for regions are available.
ObjectivesThis study aimed to describe the characteristics and independent risk factors associated with COVID-19 mortality in Castilla-La Mancha, Spain.
MethodsCohort and multicenter study in all 14 public hospitals of the Castilla-La Mancha Health Service. Baseline characteristics, preexisting comorbidities, symptoms, clinical features and treatments were included. Multivariable logistic regression was used to evaluate factors associated with death and Kaplan–Meier test to examine survival probability. Statistical significance was considered with p<0.05 (95% CI). SPSS (version 24.0 for Windows) and R 4.0.2 (R Statistics) software were used.
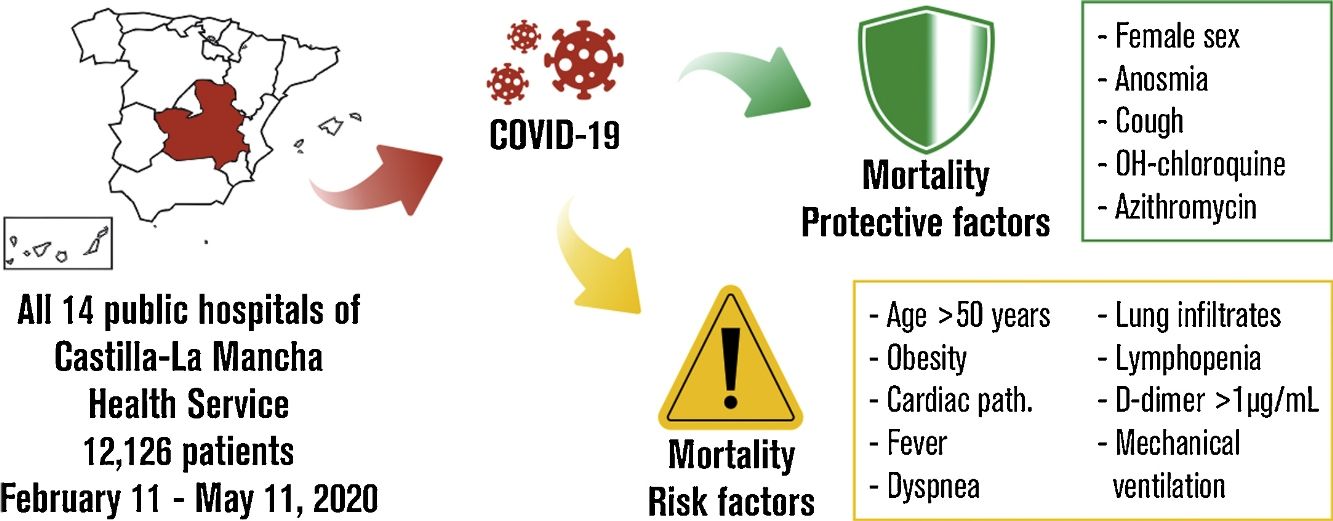
ResultsThe cohort comprised 12,126 patients sequentially attended between February 11 and May 11, 2020. The mean age of patients was 66.4 years; 5667 (46.7%) were women. Six protective factors against exitus were defined: female sex, anosmia, cough, chloroquine and azithromycin. The risk factors were: age over 50, obesity, cardiac pathology, fever, dyspnea, lung infiltrates, lymphopenia, D-dimer above 1000ng/mL, and mechanical ventilation requirement. Survival analysis showed higher survival rate in women (75.7%) than men (72.1%). Cumulative survival was 87.5% for non-hospitalized patients, 70.2% for patients admitted to hospital and 61.2% in ICU patients. Additionally, survival probability decreased with increasing age range.
ConclusionDetermination of protective or death-promoting factors could be useful to stratify patients by severity criteria and to improve COVID-19 care management.
España es uno de los países con mayor número de pacientes con COVID-19. Desafortunadamente, se dispone de pocos datos por regiones.
ObjetivosDescribir las características y los factores de riesgo independientes asociados a mortalidad por COVID-19 en Castilla-La Mancha, España.
MétodosEstudio de cohorte, multicéntrico de los 14 hospitales públicos de Castilla-La Mancha. Se evaluaron las características clínicas, comorbilidades preexistentes, síntomas y tratamientos. Se utilizó una regresión logística multivariable para evaluar los factores asociados a muerte y Kaplan-Meier para medir supervivencia. Se consideró significación estadística con p < 0,05 (IC 95%). Se utilizaron los programas SPSS (versión 24.0 para Windows) y R 4.0.2 (R Statistics).
ResultadosSe estudiaron 12.126 pacientes atendidos secuencialmente entre el 11 de febrero y el 11 de mayo de 2020. La edad media fue de 66,4 años; 5.667 (46,7%) fueron mujeres. Se definieron seis factores protectores contra el exitus: sexo femenino, anosmia, tos, cloroquina y azitromicina. Los factores de riesgo fueron: edad superior a 50, obesidad, patología cardíaca, fiebre, disnea, infiltrados pulmonares, linfopenia, dímero-D > 1.000 ng/mL y necesidad de ventilación mecánica. Se observó mayor tasa de supervivencia en mujeres (75,7%) que en hombres (72,1%). La supervivencia acumulada fue del 87,5% para pacientes no hospitalizados, 70,2% para admitidos en planta hospitalaria y 61,2% en la Unidad de Cuidados Intensivos (UCI). Además, la probabilidad de supervivencia disminuyó con el aumento del rango de edad.
ConclusiónLa determinación de los factores protectores o favorecedores de muerte podría ser útil para estratificar pacientes por criterios de gravedad y mejorar la atención frente a la COVID-19.
Since its origin in Wuhan in 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has spread rapidly in many of the world's countries. Spain has one of the highest number of affected patients in the world.1,2
Given the potential severity of the disease, it is essential to study the parameters that may be affected in different population groups, to help to predict the demand for health resources and to design effective mitigation protocols.3 Some of the risk factors for severe disease and death have already been estimated in published case series,4–6 although the details of the clinical course of the disease have not yet been well described.4 Numerous demographic studies have been conducted worldwide, showing differences and similarities in clinical appearance between regions.1,7–10 This highlights the importance of conducting studies in different world-areas.11 Castilla-La Mancha is located in the center of the Iberian Peninsula, near Madrid, and has been one of the most affected regions in Spain with 18,869 confirmed COVID-19 patients since the beginning of the pandemic. Furthermore, it has one of the highest seroprevalence rates in the country (10–13.6%).2
In this study, we show data of patients admitted to all public hospitals in Castilla-La Mancha for 90 days, during the first peak of the pandemic in the region. We describe the characteristics and explore the risk factors associated with mortality, in order to improve our knowledge in the diagnosis, clinical evolution and prognosis and thus to facilitate improvements in the treatment of this disease.
MethodStudy design and participantsThis prospective, multicenter, cohort study was carried out from February 11 to May 11, 2020. It was conducted at all 14 public hospitals of the Health Service of Castilla-La Mancha (SESCAM), Spain, covering 30,680 square miles and serving to 2 million residents in urban, suburban, and rural areas. None of the hospitals were specifically designated for COVID-19 and the distribution of patients in the centers was similar to under normal conditions.
Participants were adult patient (>18 years old) transferred between hospitals or attended in the referral hospital, meeting one or more laboratory criteria and/or one or more clinical criteria of suspected COVID-19.
Laboratory criteria: Positive detection of (1) 2019-nCoV nucleic acid by real-time Polymerase Chain Reaction (PCR). (2) IgM from human serum with rapid test for SARS-CoV-2.
Clinical criteria with COVID-19: (1) Acute respiratory infection with fever, cough or dyspnea. (2) Radiographic characteristics of pneumonia, such as multiple ground-glass shadows, infiltrative shadows and consolidation in both lungs. (3) Other symptoms such as odynophagia, anosmia, ageusia, vomiting, muscle aches, diarrhea, chest pain or headaches.
Non-criteria inclusion for patients, subsequent admissions, transfers or duplicates for the same patient, and pediatric patient (<18 years old) were excluded in our study.
Data collection and definitionsGeneral Directorate of Public Health (GDPH) promoted this study and established a trained team of thirty physicians for the protocolized extraction and collection of data from electronic medical records, using a standard data form for epidemiological surveillance, within the health information system. These physicians performed this operation after a daily updating of the admitted list in each hospital. After that, three clinical coordinators supervised and checked for errors the data collection in the GDPH.
Data collection included patient demographic information, comorbidities, initial laboratory tests (first test results available), clinical symptoms and diagnoses during the hospital course and inpatient treatments. This comprised invasive ventilation (endotracheal tube) and non-invasive mechanical ventilation (helmet, total-face, oronasal or high-flow nasal oxygen). Antiretroviral treatment included 100mg lopinavir/25mg ritonavir, 200mg emtricitabine/245mg tenofovir disoproxil or 800mg darunavir/150mg cobicistat. All variables and outcomes (including time of stay, discharge, readmission and mortality) were presented at study end point. This study followed the ‘Strengthening the Reporting of Observational Studies in Epidemiology (STROBE)’ guidelines.
Statistical analysisWe reported the distribution of characteristics overall by gender and death. Continuous variables were presented as mean with standard deviation (SD) or median with interquartile range (IQR), and categorical variables as n (%). Baseline characteristics were compared using the Student's t test or Mann–Whitney's U test for continuous variables depending on the normality of distribution of the parameters (Kolmogorov–Smirnov) or the Pearson's chi-squared test for categorical variables. Multivariable logistic regression model was used to explore the risk factors associated with exitus. We calculated Kaplan–Meier survival estimates and used the log-rank test to compare groups in terms of survival. A two-sided α of less than 0.05 was considered statistically significant. Data were analyzed using SPSS software (version 24.0 for Windows, IBM, US) and represented in graphics according to R 4.0.2 (R Statistics, Vienna, Austria).
Ethical statementThis study was conducted using publicly available data released by the Health Service of Castilla-La Mancha (SESCAM); therefore, no ethical approval was needed.
ResultsTotal sample was 12,940 patients with clinical suspicion of COVID-19 who attended one of the 14 public hospitals in Castilla-La Mancha during the study period. The validated cohort was 12,126 patients, of which 9393 were admitted (596 to ICU and 8797 to hospital ward) and 2733 were sent home with follow-up in primary care (Fig. 1).

The mean (SD) age of the sample was 66.4 (17.3) years and the median were 68 years (IQR, 54–81 years). Homogeneity between sex was observed with respect to age (p=0.716). Gender distribution was 5667 (46.7%) for women and 6459 (53.3%) for men.
Length of hospital stay was 7 days (IQR, 4–12 days), with a significant difference (p<0.001) between 8 days (IQR, 5–13 days) in men and 7 days (IQR, 4–11 days) in women. Median ICU stay was 15 days (IQR, 8–25 days) and there was no difference between genders.
All patient characteristics are listed in Table 1, with total n of each variable. Mortality rate in men was higher than women (p<0.001) and fatality increased with age when establishing ten-year ranges starting from 40 (p<0.001). This means that, considering the total number of deaths, 60.4% were men compared to 39.6% who were women (p<0.001). As for pre-existing comorbidities, a higher prevalence in men than in women was observed for HBP, cardiac pathology and respiratory pathology. Regarding symptoms, men showed lower prevalence of anosmia, diarrhea and vomiting than women. However, a higher proportion of fever, dyspnea and cough were observed in men. Thorax radiography was performed in 97.7% of the participants. A higher prevalence of lung infiltrates and lymphopenia was obtained in men, as well as a D-dimer score over than 1000ng/mL. The requirement for ventilatory support (invasive or non-invasive) and the prescription of any of the treatments used, were carried out to a greater extent in men than in women.
Patient characteristics at baseline.
| Characteristics no./no. (%) | All patients | Women | Men | p-Value (men vs women)a |
|---|---|---|---|---|
| Exitus | 2020/12,126 (16.7) | 800/5667 (14.1) | 1220/6459 (18.9) | <0.001 |
| Age, years | ||||
| 18–39 | 904/12,126 (7.5) | 500/5667 (8.8) | 404/6459 (6.3) | <0.001 |
| 40–49 | 1262/12,126 (10.4) | 624/5667 (11.0) | 638/6459 (9.9) | |
| 50–59 | 2028/12,126 (16.7) | 941/5667 (16.6) | 1087/6459 (16.8) | |
| 60–69 | 2170/12,126 (17.9) | 867/5667 (15.3) | 1303/6459 (20.2) | |
| 70–79 | 2382/12,126 (19.6) | 1061/5667 (18.7) | 1321/6459 (20.5) | |
| ≥80 | 3380/12,126 (27.9) | 1674/5667 (29.5) | 1706/6459 (26.4) | |
| Preexisting comorbidities | ||||
| HBP | 6276/12,114 (51.8) | 2857/5659 (50.5) | 3419/6455 (53) | 0.006 |
| Obesity | 2100/11,186 (18.8) | 967/5280 (18.3) | 1133/5906 (19.2) | 0.240 |
| Cardiac pathology | 3006/12,109 (24.8) | 1236/5657 (21.8) | 1770/6452 (27.4) | <0.001 |
| Respiratory pathology | 2735/12,099 (22.6) | 1085/5652 (19.2) | 1650/6447 (25.6) | <0.001 |
| Symptoms | ||||
| Anosmia | 653/12,119 (5.4) | 367/5663 (6.5) | 286/6456 (4.4) | <0.001 |
| Diarrhea | 2048/12,121 (16.9) | 1066/5664 (18.8) | 982/6457 (15.2) | <0.001 |
| Vomiting | 899/12,121 (7.4) | 543/5664 (9.6) | 356/6457 (5.5) | <0.001 |
| Fever | 7543/12,120 (62.2) | 3240/5663 (57.2) | 4303/6457 (66.6) | <0.001 |
| Dyspnea | 6870/12,121 (56.7) | 3110/5664 (54.9) | 3760/6457 (58.2) | <0.001 |
| Cough | 6829/12,120 (56.3) | 3109/5663 (54.9) | 3720/6457 (57.6) | 0.003 |
| Clinical features | ||||
| Lung infiltrations | 8921/11,873 (75.1) | 3828/5507 (69.5) | 5093/6366 (80) | <0.001 |
| Lymphopenia | 6629/11,565 (57.3) | 2781/5324 (52.2) | 3848/6241 (61.7) | <0.001 |
| D-dimer≥1000ng/mL | 4436/10,191 (43.5) | 1928/4610 (41.8) | 2508/5581 (44.9) | 0.002 |
| Treatments | ||||
| Invasive ventilation | 530/12,126 (4.4) | 174/5667 (3.1) | 356/6459 (5.5) | <0.001 |
| Non-invasive ventilation | 764/12,124 (6.3) | 291/5667 (5.1) | 437/6457 (7.3) | <0.001 |
| Antiretroviral treatment | 3337/12,124 (27.5) | 1262/5666 (22.3) | 2075/6458 (32.1) | <0.001 |
| Chloroquine | 7910/12,124 (65.2) | 3410/5666 (60.2) | 4500/6458 (69.7) | <0.001 |
| Interferon β-1b | 292/12,123 (2.4) | 89/5666 (1.6) | 203/6457 (3.1) | <0.001 |
| Azithromycin | 7741/12,120 (63.9) | 3431/5665 (60.6) | 4310/6455 (66.8) | <0.001 |
| Corticosteroids | 4785/12,119 (39.5) | 1862/5664 (32.9) | 2923/6455 (45.3) | <0.001 |
| Tocilizumab | 370/12,118 (3.1) | 120/5664 (2.1) | 250/6454 (3.9) | <0.001 |
HBP: high blood pressure.
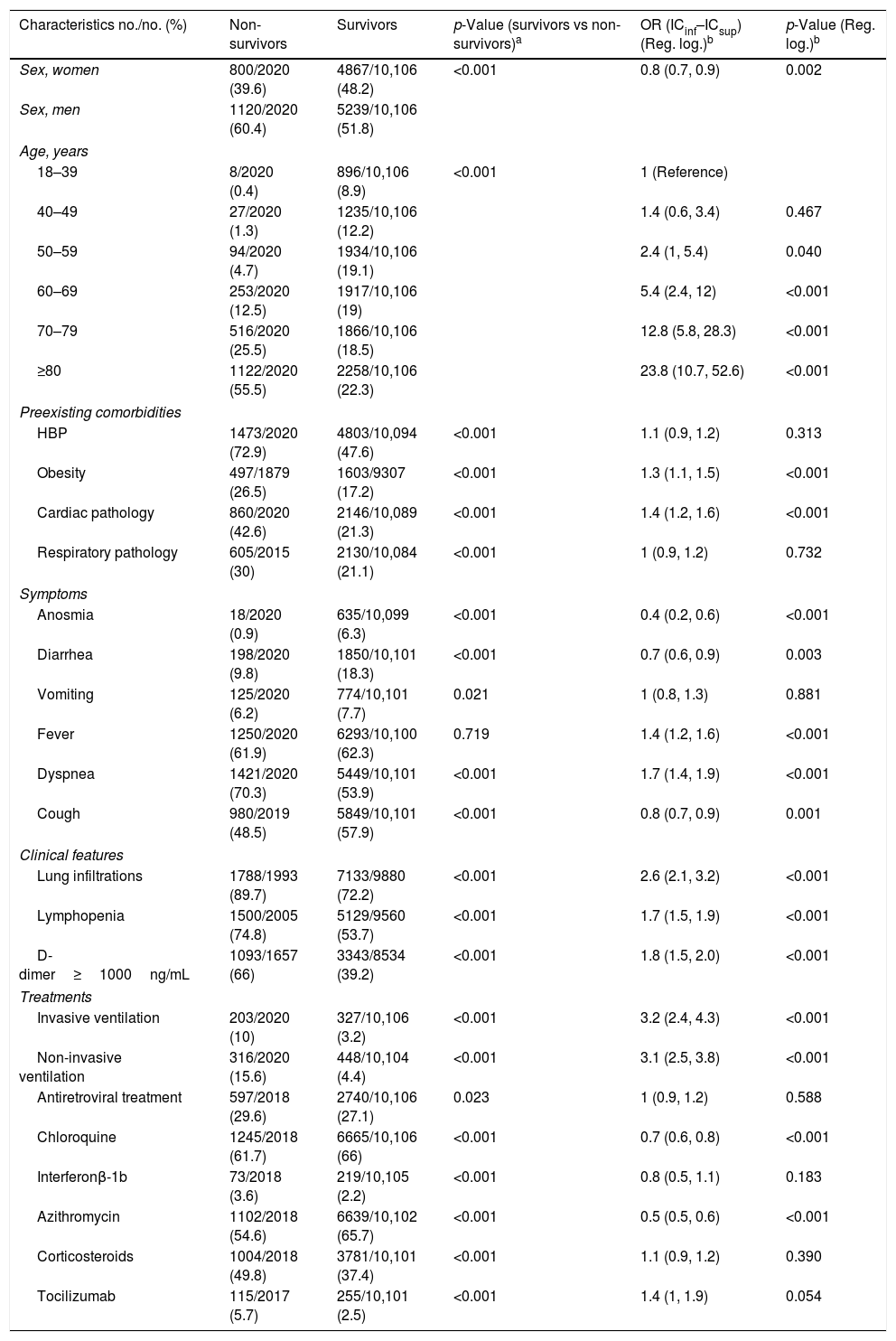
Comparison between survivors and non-survivors for each study variable is presented in Table 2. There was a higher proportion of deaths among men than women. This fact increased with age. The deceased showed a higher prevalence of pre-existing comorbidities. Regarding symptoms, there was a higher prevalence of dyspnea in non-survivors. However, a higher proportion of anosmia, diarrhea, vomiting and coughing was observed in survivors. The clinical features of the non-survivors were significantly worse than survivors.
Bivariable and multivariable-adjusted risk model for exitus (non-survivors).
| Characteristics no./no. (%) | Non-survivors | Survivors | p-Value (survivors vs non-survivors)a | OR (ICinf–ICsup) (Reg. log.)b | p-Value (Reg. log.)b |
|---|---|---|---|---|---|
| Sex, women | 800/2020 (39.6) | 4867/10,106 (48.2) | <0.001 | 0.8 (0.7, 0.9) | 0.002 |
| Sex, men | 1120/2020 (60.4) | 5239/10,106 (51.8) | |||
| Age, years | |||||
| 18–39 | 8/2020 (0.4) | 896/10,106 (8.9) | <0.001 | 1 (Reference) | |
| 40–49 | 27/2020 (1.3) | 1235/10,106 (12.2) | 1.4 (0.6, 3.4) | 0.467 | |
| 50–59 | 94/2020 (4.7) | 1934/10,106 (19.1) | 2.4 (1, 5.4) | 0.040 | |
| 60–69 | 253/2020 (12.5) | 1917/10,106 (19) | 5.4 (2.4, 12) | <0.001 | |
| 70–79 | 516/2020 (25.5) | 1866/10,106 (18.5) | 12.8 (5.8, 28.3) | <0.001 | |
| ≥80 | 1122/2020 (55.5) | 2258/10,106 (22.3) | 23.8 (10.7, 52.6) | <0.001 | |
| Preexisting comorbidities | |||||
| HBP | 1473/2020 (72.9) | 4803/10,094 (47.6) | <0.001 | 1.1 (0.9, 1.2) | 0.313 |
| Obesity | 497/1879 (26.5) | 1603/9307 (17.2) | <0.001 | 1.3 (1.1, 1.5) | <0.001 |
| Cardiac pathology | 860/2020 (42.6) | 2146/10,089 (21.3) | <0.001 | 1.4 (1.2, 1.6) | <0.001 |
| Respiratory pathology | 605/2015 (30) | 2130/10,084 (21.1) | <0.001 | 1 (0.9, 1.2) | 0.732 |
| Symptoms | |||||
| Anosmia | 18/2020 (0.9) | 635/10,099 (6.3) | <0.001 | 0.4 (0.2, 0.6) | <0.001 |
| Diarrhea | 198/2020 (9.8) | 1850/10,101 (18.3) | <0.001 | 0.7 (0.6, 0.9) | 0.003 |
| Vomiting | 125/2020 (6.2) | 774/10,101 (7.7) | 0.021 | 1 (0.8, 1.3) | 0.881 |
| Fever | 1250/2020 (61.9) | 6293/10,100 (62.3) | 0.719 | 1.4 (1.2, 1.6) | <0.001 |
| Dyspnea | 1421/2020 (70.3) | 5449/10,101 (53.9) | <0.001 | 1.7 (1.4, 1.9) | <0.001 |
| Cough | 980/2019 (48.5) | 5849/10,101 (57.9) | <0.001 | 0.8 (0.7, 0.9) | 0.001 |
| Clinical features | |||||
| Lung infiltrations | 1788/1993 (89.7) | 7133/9880 (72.2) | <0.001 | 2.6 (2.1, 3.2) | <0.001 |
| Lymphopenia | 1500/2005 (74.8) | 5129/9560 (53.7) | <0.001 | 1.7 (1.5, 1.9) | <0.001 |
| D-dimer≥1000ng/mL | 1093/1657 (66) | 3343/8534 (39.2) | <0.001 | 1.8 (1.5, 2.0) | <0.001 |
| Treatments | |||||
| Invasive ventilation | 203/2020 (10) | 327/10,106 (3.2) | <0.001 | 3.2 (2.4, 4.3) | <0.001 |
| Non-invasive ventilation | 316/2020 (15.6) | 448/10,104 (4.4) | <0.001 | 3.1 (2.5, 3.8) | <0.001 |
| Antiretroviral treatment | 597/2018 (29.6) | 2740/10,106 (27.1) | 0.023 | 1 (0.9, 1.2) | 0.588 |
| Chloroquine | 1245/2018 (61.7) | 6665/10,106 (66) | <0.001 | 0.7 (0.6, 0.8) | <0.001 |
| Interferonβ-1b | 73/2018 (3.6) | 219/10,105 (2.2) | <0.001 | 0.8 (0.5, 1.1) | 0.183 |
| Azithromycin | 1102/2018 (54.6) | 6639/10,102 (65.7) | <0.001 | 0.5 (0.5, 0.6) | <0.001 |
| Corticosteroids | 1004/2018 (49.8) | 3781/10,101 (37.4) | <0.001 | 1.1 (0.9, 1.2) | 0.390 |
| Tocilizumab | 115/2017 (5.7) | 255/10,101 (2.5) | <0.001 | 1.4 (1, 1.9) | 0.054 |
HBP: high blood pressure.
In the multiple logistic regression model (Fig. 2) it was observed that female sex, anosmia, diarrhea, cough, OH-chloroquine and azithromycin acted as protective factors against exitus by COVID-19. The risk factors that increased the probability of death were: male sex, age over 50 years, obesity, cardiac disease, fever, dyspnea, pulmonary infiltrates, lymphopenia, D-dimer above 1000ng/mL and mechanical ventilation (invasive and non-invasive).
. OR: odds ratio; HBP: high blood pressure.")
Cumulative observation time was 387,610 patient-days from the arrival of the patients at the hospital to end of follow-up for the 12,126 patients. Median follow-up was 35 days (IQR, 21–45 days). A median of 74 patients per day were treated (IQR, 10–246 patients per day) with a median of 11 deaths per day (IQR, 2–40 deaths per day). Mortality rate was 5.2 per 1000 patient-days (IQR, 4.8–5.6 per 1000 patient-days). A survival analysis was performed for all patients during the 90-day follow-up (Fig. 3A). Higher mortality was recorded in the first 10 days (up to 12.5%). The maximum mortality was 20.2% and was recorded on day 62. Cumulative survival between gender was compared on Fig. 3B, with a higher survival rate in women (blue, 75.7%) than in men (red, 72.1%), which made a significant difference in the log-rank test (p<0.001). In Fig. 3C, survival was segmented according to hospital/ICU stay or homebound patients. The cumulative survival of patients sent home (in red) was 87.5%. Patients admitted to hospital (green) had a cumulative survival of 70.2% and those admitted to ICU (blue) of 61.2%. The log-rank test showed significant differences between the three groups (p<0.001). Finally, Fig. 3D shows how survival probability decreased with increasing age range (p<0.001).
Discussion Without distinctions. (B) By gender. (C) According to admission. (D) By age range.")
We analyzed consecutive data from patients who were hospitalized in the region of Castilla-La Mancha, one of the most affected and prevalent areas of COVID-19 in Spain during the first peak of the pandemic.2 In Spain, duties for health care are transferred to the Autonomous Communities where the same public health protocols are followed. This work is one of the largest studies carried out in a multicentric way within the same health system (the 14 public hospitals of the Health Service of Castilla-La Mancha), which allows the homogenization and consistency of the data and reduces the possibility of local biases caused by the idiosyncrasy of each hospital.
The median age of our sample was 68 years, slightly lower than other studies carried out in Spain,1,10 Italy9 or United Kingdom,12 but higher than other reports from China,4,5,13 the US8 or Spain.7 As in the series of patients from the United Kingdom studied by Docherty et al. and in Spain by Berenguer et al., mortality of our patients was also higher in men than women. It has been argued that differences in sex-specific mechanisms such as hormone-regulated expression of genes like angiotensin converting enzyme (ACE) 2 receptor and TMPRSS2, as well as sex hormone-driven innate and adaptive immune responses could justify these differences and should be better studied.14
Moreover, in our study case fatality rates were significantly higher in age ranges above 40 years like in Spain, UK or Italy.7,12,15
The series of Richardson et al. from the US showed higher percentages than this work in terms of hypertension and obesity.8 However, in other studies carried out in Spain, China and the United Kingdom the percentages were similar or lower.4,7,12
As in previous studies from UK or other regions of Spain, we have found that some symptoms and comorbidities increase the risk of exitus, such as obesity, cardiac pathology,12 fever or dyspnea.7,10 Moreover, in our work we could observe that anosmia, diarrhea and cough were related to low rates of mortality. This could justify the low percentage of these symptoms found in our cohort, as it is mainly composed by severe patients who came to the hospital. Therefore, the patient's symptoms could help us to stratify the severity of COVID-19 patients on health care demand.
The D-dimer average level of our patients is above most national1 and international4 series, which is indicative of the severity of the patients included in this work.16 In our cohort we can establish as associated factors of exitus: lung infiltrates, lymphopenia and D-dimer>1000ng/ml. Other studies1,7,17,18 from Spain, China and USA, found similar results with different mortality rates, supporting the existence of a severe COVID-19 patient profile. In this terms, Yong Gao et al.19 determined that combined detection of clinical parameters may have greater specificity and sensitivity for early prediction of the severity of COVID-19 patients, which has important clinical value.
In our study, we found higher mortality rates in those patients who required invasive (p<0.001) and non-invasive ventilation (p<0.001), since these patients showed greater severity of their acute respiratory syndrome (ARDS) and required admission to ICUs. Notwithstanding, our results are in line with those described in the literature from other regions of Spain, China and USA.20–22
At the beginning of the pandemic in Spain, only symptomatic treatment was indicated. Later, most of our patients underwent treatments that allegedly have antiviral activity against SARS-CoV-2. Different treatments have changed during the course of the pandemic, but they were always based on the indications of the Spanish Ministry of Health and the availability of treatments.
In our study we found a significant difference in the survival of patients who were treated with chloroquine (p<0.001) and azithromycin (p<0.001). Recently, in a multinational registry analysis23 no benefit of hydroxychloroquine or chloroquine (used alone or with a macrolide) could be confirmed in the hospital outcomes for COVID-19. These drug regimens were associated with decreased in-hospital survival and increased frequency of ventricular arrhythmias when used for the treatment of COVID-1924–28 so they have been subsequently retracted.23 Therefore, it is necessary to gain more randomized controlled trial evidence prior to the incorporation of hydroxychloroquine and azithromycin into treatment guidelines. Like in other studies, the use of these antiretroviral treatments,29 anti-inflammatory cytokines (i.e. interferon)30 or Tocilizumab31 did not demonstrate a significant decrease in mortality in our study population (Table 2).
It has been reported that an early short course of corticosteroids in patients with moderate to severe COVID-19 improved clinical outcomes. In fact, its use has been implemented for the treatment of COVID-19.32–34 However, for patients with severe COVID-19 but without ARDS, confirmation regarding benefit from different bodies of evidence is inconsistent and of very low quality.35 In our work, no significant differences were found, possibly due to the lack of standardization in dose and timing of corticosteroids administration.
A higher and earlier mortality rate was observed in patients admitted to hospital, which stabilized from approximately day 10 (Fig. 3C). The ICU survival probability reduces later than the hospital mortality rate during the time of admission, but faster than the hospital mortality from day 23. This may be due to the increased medical attention received by ICU patients, which kept them alive in the first few days in higher proportion than patients on the hospital ward.36
Mortality rate in our cohort was lower than in other regions of the US,8 UK,12 Spain1,7 and China4 but higher than in other studies also developed in China or Italy.1,9,37 The variations in the different mortality rates could be due to the preferential inclusion of severe cases during the maximum emergency situation which could correspond to the profile of people seeking medical care and therefore lead to a fatal outcome.3 Moreover, mortality rates discrepancies may be due to differences in each health care system and data collection.
We acknowledge some limitations. First, it could not be confirmed by laboratory testing that all patients were positive for PCR due to the collapse of the health system. Second, the final date of the study was May 11. The status of all patients was reviewed on that date. There was no follow-up after this date, so the mortality rate could be higher and was not recorded later. Third, the high prevalence of the disease led to priority being given to the care of the most severe patients. This could lead to a selection bias in the study. And fourth, we had no data about the asymptomatic population and patients admitted to Senior Citizen's Residences in Castilla-La Mancha, so we could not show a broader frame of the pandemic in our region.
On the other hand, this study has several strengths. We included all patients from the 14 public hospitals in Castilla-La Mancha during the period of highest COVID-19 impact. All the centers are under the same health management system with the same protocols (competence-based health management is transferred to the autonomous communities). This implies homogeneity in the clinical patterns applied, which guarantees the homogeneity of the data. In addition, the large sample size favors the definition of the characteristics of our region, one of the most affected in the country.
To conclude, the study and determination of protective or death-promoting factors could be useful to stratify patients by severity criteria to improve COVID-19 care management. More studies of this type are needed to focus on health promotion, prevention, diagnosis, management, and future treatment, since demographic, racial, social, genetic and health policy conditions determine the evolution of this disease and population health. These results could help us to tackle future pandemic waves and prevent premature deaths.11,38 Therefore, clinical trials and systematic reviews are needed to assess the beneficial and harmful effects of pharmacological and other interventions to confront this high-prevalence disease.
FundingThis work is supported by the Spanish Ministry of Health and the General Directorate of Public Health of Castilla-La Mancha. Leticia Serrano-Oviedo is the recipient of a contract made by the Directorate of Public Health of Castilla-La Mancha specifically devoted to study the COVID-19 pandemic.
Conflict of interestThe authors have no conflict of interest to declare.
We thank all health-care workers involved in the diagnosis and treatment of patients in Castilla-La Mancha. We also acknowledge the COVID-19 SESCAM Network and all the public hospitals engaged in this study.
Coordination: Authors who sign this work, Jesús Fernández Sanz, Juan José Camacho, Luis Morell, Desirée Bustos, Paloma García.
General Hospital of Alcázar de San Juan: Lucas Salcedo, Óscar Talavera, Ángel Arias, Jaime Bustos, Irene Sánchez.
General Hospital of Almansa: Antonio Sánchez, Leire Sogorb.
General Hospital of Cuenca: Ángel Pérez Sola, María Obispo, Rodrigo López.
General Hospital of Guadalajara: Antonio Sanz, Lourdes Prats, Miriam Aguado, Pablo Solano.
General Hospital of Hellín: Carlos Castillo, Marina Martínez.
General Hospital of Manzanares: Nuria Sánchez, Ana I. Sánchez-Migallón.
General Hospital of Puertollano: Cesáreo Peco, Beatriz del Hoyo, Altea Montalbán.
General Hospital of Talavera de la Reina: José María Ruiz, Inés Rodríguez.
General Hospital of Tomelloso: Silvia Quemada, Pedro J. Izquierdo.
General Hospital of Valdepeñas: Damián Aranda, Lucía Sampériz, María Gallego.
General Hospital of Villarrobledo: Caridad Ballesteros, Miguel Toledo, Víctor Manuel León.
SESCAM Central Services: Regina Leal, José Antonio Ballesteros, Iñigo Cortázar, Begoña Fernández, José Sacristán, Pedro López.
University General Hospital of Albacete: Ibrahim Hernández, Inmaculada Tendero, Mª José Blázquez, Cristina Mora, Ana Utiel.
University General Hospital of Ciudad Real: Alberto Jara, Ana Sofía Yuste, Víctor Baladrón, Rubén Villazala, Alfonso Hernández, Natalia Bejarano, Marian Montero, Gema Verdugo, Rubén Bernal, Elena Ávila, Patricia Reina.
University General Hospital of Toledo: Juan Blas, Laura López, Alberto López, Jaime López, Mª Teresa Rodríguez.







