

Paradoxes are usually instructive, and philosophers use them to reveal the complexity of reality. On a global level, there is a striking paradox between human health and planetary health. The human animal broadly enjoys very good health. There are already 7.5 billion of us, and numbers continue to grow.1 We are extremely long-lived,2 if not to biblical standards, but it seems we are arriving at our limits in terms of age.3 Extreme poverty, infant and neonatal mortality, and death rates from infections and chronic diseases are also falling dramatically. However, the ecological balance and natural systems are suffering. Human health is improving at the expense of increased pollution, reduced biodiversity, loss of rainforests and other environmental lungs, and global warming. The quantity and quality of this growth of human health is neither sustainable over time, nor is it compatible with the health of the planet.
Planetary health is a new concept that emerged in 2014.4 It refers to the health of human civilization now and in the future, and depends, of course, on the complete physical, mental and social welfare of the population, but also on the state of the natural systems that sustain us. It implies, then, social, economic and environmental health determinants. Basically, this paradigm shift reminds us that we cannot continue to exploit nature as we have been doing until now, as everything is interconnected. The problems of the planet directly or indirectly cause human disease, and the solutions that benefit the planet must also benefit human health (Fig. 1).

Ecosystems are currently being destroyed at a rate unprecedented in history. For 12000 years, following the introduction of writing and the development of civilizations, humans have been considered to live in the Holocene period. Now, however, it has been suggested that we are already living in the Anthropocene,5 an age in which humans are changing the planet. This new epoch began scarcely 200 years ago, from the beginning of the 1800s, when evidence already emerged of an increase in the temperature of the oceans caused by humans, along with growing ocean acidification, overfishing, overuse of dosmesticated land, requiring overuse of fertilizers, increased emissions of atmospheric pollutants, etc. This vision of ecosystems is not catastrophic, it is realistic; and the solution to poor planetary health is Planetary Medicine, partly based on chaos theory, by which small changes can, in a non-deterministic and non-linear fashion, produce major worldwide upheavals; and it is also based on the Gaia theory, which proposes that Earth is a living, self-regulating organism that balances and perpetuates life. However, these mechanisms have a breaking point, and we can and must, individually and collectively, help them survive.6,7
Nevertheless, improvements in global world health do not, at the moment, extend to respiratory health. The WHO includes 5 respiratory diseases (COPD, pneumonia, lung cancer, sleep apnea, and tuberculosis) in the list of the 10 top causes of global mortality.8 There are 334 million asthmatics, 323 million COPD patients, and 1.1 billion smokers, more than at any other time in history.9 Since the mortality rates of many respiratory diseases are falling, respiratory patients are living longer. As a species, our breathing is becoming increasingly poor, and moreover, we are breathing poor quality air.
Solutions to planetary respiratory diseases must begin at an individual level – not only with individualized medicine, but also with more global and social medicine, practiced from a population approach.10 Current attitudes to healthcare – curative, biomedical, molecular and highly personalized – must be changed to accommodate, or at least complement, the root environmental and social causes of today's diseases.
We need to take a preventive approach: active lifestyles with age-appropriate exercise for each individual, a Mediterranean diet, moderate alcohol consumption, no smoking, scheduled vaccination and screening programs, and to encourage individuals to try to be happy and transcendent. The key lies in sustainable growth.
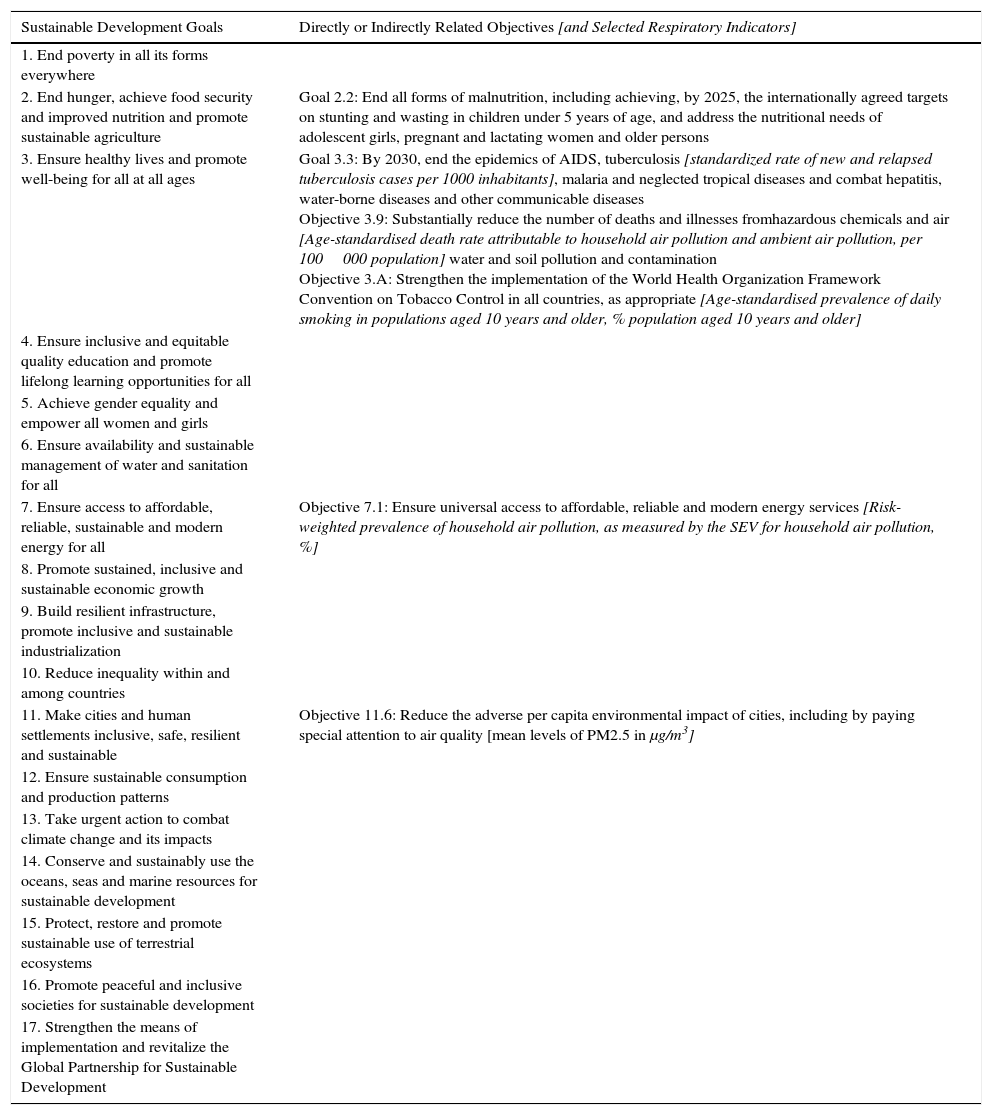
In September 2015, the United Nations identified 17 objectives for sustainable growth (Table 1),11 as an extension of their Millennium health objectives, adding some additional aspects associated with education, individual risk factors, per capita income of the country, and other more environmental issues, such as protection of the oceans and forests, the fight against climate change, and biodiversity. On September 22, 2016, the first assessment of these objectives was conducted, in which Spain was found to have made excellent progress. The recent (2015) report on Objectives for Sustainable Development placed us in a very respectable 7th position among the 188 countries evaluated.12 However, this achievement may be ephemeral if our respiratory performance does not improve on the following three levels. On the healthcare level: the prevalence of smoking among the population must be reduced, not only by increasing the number of individuals who stop smoking, but also preventing young people from taking up the habit,11 and tuberculosis, AIDS, and other communicable respiratory diseases must be controlled. On the infrastructure level: free, universal access to healthcare and education must be maintained. And on the environmental level: pollution, both in the environment and indoor, must be reduced, and actions must be taken to combat climate change and its impact (Table 1). These indicators underline the importance of committing to and working toward changes promoting healthy lifestyles, improving infrastructures, reducing pollution, and enhancing the quality of life and respiratory health of our society.13,14
Directly or Indirectly Related WHO Sustainable Development Goals for 2030 [and Selected Respiratory Indicators].
| Sustainable Development Goals | Directly or Indirectly Related Objectives [and Selected Respiratory Indicators] |
|---|---|
| 1. End poverty in all its forms everywhere | |
| 2. End hunger, achieve food security and improved nutrition and promote sustainable agriculture | Goal 2.2: End all forms of malnutrition, including achieving, by 2025, the internationally agreed targets on stunting and wasting in children under 5 years of age, and address the nutritional needs of adolescent girls, pregnant and lactating women and older persons |
| 3. Ensure healthy lives and promote well-being for all at all ages | Goal 3.3: By 2030, end the epidemics of AIDS, tuberculosis [standardized rate of new and relapsed tuberculosis cases per 1000 inhabitants], malaria and neglected tropical diseases and combat hepatitis, water-borne diseases and other communicable diseases Objective 3.9: Substantially reduce the number of deaths and illnesses fromhazardous chemicals and air [Age-standardised death rate attributable to household air pollution and ambient air pollution, per 100000 population] water and soil pollution and contamination Objective 3.A: Strengthen the implementation of the World Health Organization Framework Convention on Tobacco Control in all countries, as appropriate [Age-standardised prevalence of daily smoking in populations aged 10 years and older, % population aged 10 years and older] |
| 4. Ensure inclusive and equitable quality education and promote lifelong learning opportunities for all | |
| 5. Achieve gender equality and empower all women and girls | |
| 6. Ensure availability and sustainable management of water and sanitation for all | |
| 7. Ensure access to affordable, reliable, sustainable and modern energy for all | Objective 7.1: Ensure universal access to affordable, reliable and modern energy services [Risk-weighted prevalence of household air pollution, as measured by the SEV for household air pollution, %] |
| 8. Promote sustained, inclusive and sustainable economic growth | |
| 9. Build resilient infrastructure, promote inclusive and sustainable industrialization | |
| 10. Reduce inequality within and among countries | |
| 11. Make cities and human settlements inclusive, safe, resilient and sustainable | Objective 11.6: Reduce the adverse per capita environmental impact of cities, including by paying special attention to air quality [mean levels of PM2.5 in μg/m3] |
| 12. Ensure sustainable consumption and production patterns | |
| 13. Take urgent action to combat climate change and its impacts | |
| 14. Conserve and sustainably use the oceans, seas and marine resources for sustainable development | |
| 15. Protect, restore and promote sustainable use of terrestrial ecosystems | |
| 16. Promote peaceful and inclusive societies for sustainable development | |
| 17. Strengthen the means of implementation and revitalize the Global Partnership for Sustainable Development |
Examples of success include the Montreal protocol of 1987,15 the aim of which was to reduce/eliminate the greenhouse gases damaging the ozone layer and led to the replacement of CFC propellants by HFA in the majority of metered dose inhalers for respiratory diseases. The objective was achieved before the planned date. We have to seek out and identify more examples of good practice in Respiratory Planetary Medicine.
Respiratory medicine specialists and translational respiratory clinical scientists have and will continue to have ample opportunities, in both national and international research programs. But such translation cannot only be from the test-tube or the animal to the patient, nor can it be limited to Public Health: definitive translational medicine must have an impact on Respiratory Planetary Health. Planetary pulmonologists are needed, experts who care as much for their patients’ lungs as for the welfare of natural systems and their impact on future generations.
FundingHorizon 2020 HCO 2015 Grant Agreement Number 681040 TackSHS.
Conflict of InterestsThe authors declare that they have no conflict of interests directly or indirectly related with the contents of this manuscript.
We thank our colleagues on the European project Tackling second hand tobacco smoke and e-cigarette emissions: exposure assessment, novel interventions, impact on lung diseases and economic burden in diverse European populations for discussing the issues addressed in this manuscript. The TackSHS Project.
Please cite this article as: Soriano JB, Soriano C, Fernández E. Medicina planetaria respiratoria. Arch Bronconeumol. 2017;53:297–299.







